UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
______________________________
FORM 10-K
(Mark One)
☒ ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934
For the fiscal year ended December 31, 2019
or
☐ TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934
For the transition period from ________________ to __________________.
Commission file number: 001-36291
____________________
DIAMEDICA THERAPEUTICS INC.
(Exact name of registrant as specified in its charter)
____________________
|
British Columbia (State or other jurisdiction of incorporation or organization) |
Not Applicable (I.R.S. Employer Identification No.) |
|
Two Carlson Parkway, Suite 260 Minneapolis, Minnesota (Address of principal executive offices) |
55447 (Zip Code) |
Registrant’s telephone number, including area code: (763) 612-6755
Securities registered pursuant to Section 12(b) of the Act:
|
Title of each class |
Trading Symbol(s) |
Name of each exchange on which registered |
|
Voting Common Shares, no par value per share |
DMAC |
The Nasdaq Capital Market The Nasdaq Stock Market LLC |
Securities registered pursuant to Section 12(g) of the Act: None
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. YES ☐ NO ☒
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Act. YES ☐ NO ☒
Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. YES ☒ NO ☐
Indicate by check mark whether the registrant has submitted electronically every Interactive Data File required to be submitted pursuant to Rule 405 of Regulation S-T (§ 232.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit such files). YES ☒ NO ☐
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, a smaller reporting company or an emerging growth company. See definitions of “large accelerated filer,” “accelerated filer,” “smaller reporting company” and “emerging growth company” in Rule 12b-2 of the Exchange Act.
|
Large accelerated filer ☐ |
Accelerated filer ☐ |
Non-accelerated filer ☒ |
Smaller reporting company ☒ |
|
Emerging growth company ☒ |
If an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. ☒
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Act). YES ☐ NO ☒
The aggregate market value of the registrant’s voting common shares held by non-affiliates, computed by reference to the closing sales price at which the voting common shares were last sold as of June 30, 2019 (the last business day of the registrant’s most recently completed second fiscal quarter), as reported by the Nasdaq Capital Market on that date, was $53.4 million.
As of March 20, 2020, there were 14,139,074 voting common shares outstanding.
DOCUMENTS INCORPORATED BY REFERENCE
Part III of this Annual Report on Form 10-K incorporates by reference information (to the extent specific sections are referred to herein) from the registrant’s Proxy Statement for its 2020 Annual General Meeting of Shareholders to be held June 2, 2020.
[page intentionally left blank]
DIAMEDICA THERAPEUTICS INC.
ANNUAL REPORT ON FORM 10-K
FISCAL YEAR ENDED DECEMBER 31, 2019
TABLE OF CONTENTS
| Page | ||
| CAUTIONARY NOTE REGARDING FORWARD-LOOKING STATEMENTS | 1 | |
| INDUSTRY AND MARKET DATA | 2 | |
| PART I | 3 | |
| Item 1. | Business | 3 |
| Information About Our Executive Officers | 27 | |
| Item 1A. | Risk Factors | 29 |
| Item 2. | Properties | 69 |
| Item 3. | Legal Proceedings | 69 |
| Item 4. | Mine Safety Disclosures | 70 |
| PART II | 71 | |
| Item 5. | Market for Registrant’s Common Equity, Related Stockholder Matters and Issuer Purchases of Equity Securities | 71 |
| Item 6. | Selected Financial Data | 82 |
| Item 7. | Management’s Discussion and Analysis of Financial Condition and Results of Operations | 83 |
| Item 7A. | Quantitative and Qualitative Disclosures About Market Risk | 94 |
| Item 8. | Financial Statements and Supplementary Data | 95 |
| Item 9. | Changes In and Disagreements With Accountants on Accounting and Financial Disclosure | 120 |
| Item 9A. | Controls and Procedures | 120 |
| Item 9B. | Other Information | 121 |
| PART III | 122 | |
| Item 10. | Directors, Executive Officers and Corporate Governance | 122 |
| Item 11. | Executive Compensation | 122 |
| Item 12. | Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters | 122 |
| Item 13. | Certain Relationships and Related Transactions, and Director Independence | 123 |
| Item 14. | Principal Accounting Fees and Services | 123 |
| PART IV | 124 | |
| Item 15. | Exhibits, Financial Statement Schedules | 124 |
| Item 16. | Form 10-K Summary | 129 |
| SIGNATURES | 130 | |
_____________
This annual report on Form 10-K contains certain forward-looking statements that are within the meaning of Section 27A of the United States Securities Act of 1933, as amended, and Section 21E of the United States Securities Exchange Act of 1934, as amended, and are subject to the safe harbor created by those sections. For more information, see “Cautionary Note Regarding Forward-Looking Statements.”
As used in this report, references to “DiaMedica,” the “Company,” “we,” “our” or “us,” unless the context otherwise requires, refer to DiaMedica Therapeutics Inc. and its subsidiaries, all of which are consolidated in DiaMedica’s consolidated financial statements. References in this report to “common shares” means our voting common shares, no par value per share.
We own various unregistered trademarks and service marks, including our corporate logo. Solely for convenience, the trademarks and trade names in this report are referred to without the ® and ™ symbols, but such references should not be construed as any indicator that the owner of such trademarks and trade names will not assert, to the fullest extent under applicable law, their rights thereto. We do not intend the use or display of other companies’ trademarks and trade names to imply a relationship with, or endorsement or sponsorship of us by, any other companies.
CAUTIONARY NOTE REGARDING FORWARD-LOOKING STATEMENTS
Statements in this annual report on Form 10-K that are not descriptions of historical facts are forward-looking statements within the meaning of the United States Private Securities Litigation Reform Act of 1995 that are based on management’s current expectations and are subject to risks and uncertainties that could negatively affect our business, operating results, financial condition and share price. We have attempted to identify forward-looking statements by terminology including “anticipates,” “believes,” “can,” “continue,” “could,” “estimates,” “expects,” “intends,” “may,” “plans,” “potential,” “predicts,” “should,” “will,” “would,” the negative of these terms or other comparable terminology, and the use of future dates.
The forward-looking statements in this report include, among other things, statements about:
|
● |
our plans to develop, obtain regulatory approval for and commercialize our DM199 product candidate for the treatment of CKD and AIS and our expectations regarding the benefits of our DM199 product candidate; |
|
● |
our ability to conduct successful clinical testing of our DM199 product candidate for CKD and AIS; |
|
● |
our ability to obtain required regulatory approvals of our DM199 product candidate for CKD and AIS; |
|
● |
the perceived benefits of our DM199 product candidate over existing treatment options for CKD and AIS; |
|
● |
the potential size of the markets for our DM199 product candidate and our ability to serve those markets; |
|
● |
the rate and degree of market acceptance, both in the United States and internationally, of our DM199 product candidate for CKD and AIS; |
|
● |
our ability to partner with and generate revenue from biopharmaceutical or pharmaceutical partners to develop, obtain regulatory approval for and commercialize our DM199 product candidate for CKD and AIS.; |
|
● |
the success, cost and timing of planned clinical trials, as well as our reliance on collaboration with third parties to conduct our clinical trials; |
|
● |
our commercialization, marketing and manufacturing capabilities and strategy; |
|
● |
expectations regarding federal, state, and foreign regulatory requirements and developments, such as potential United States Food and Drug Administration (FDA) regulation of our DM199 product candidate for CKD and AIS; |
|
● |
expectations regarding competition and our ability to obtain data exclusivity for our DM199 product candidate for CKD and AIS; |
|
● |
our ability to obtain funding for our operations, including funding necessary to complete planned clinical trials and obtain regulatory approvals for our DM199 product candidate for CKD and AIS; |
|
● |
our estimates regarding expenses, future revenue, capital requirements and needs for additional financing; |
|
● |
our expectations regarding our ability to obtain and maintain intellectual property protection for our DM199 product candidate; and |
|
● |
our anticipated use of the net proceeds from our December 2018 initial public offering in the United States and our February 2020 underwritten public offering. |
These forward-looking statements are subject to a number of risks, uncertainties and assumptions, including those described under “Part I. Item 1A. Risk Factors in this report. Moreover, we operate in a very competitive and rapidly-changing environment. New risks emerge from time to time. It is not possible for our management to predict all risks, nor can we assess the impact of all factors on our business or the extent to which any factor, or combination of factors, may cause actual results to differ materially from those contained in any forward-looking statements we may make. In light of these risks, uncertainties and assumptions, the forward-looking events and circumstances discussed in this report may not occur and actual results could differ materially and adversely from those anticipated or implied in the forward-looking statements. Forward-looking statements should not be relied upon as predictions of future events. Although we believe that the expectations reflected in the forward-looking statements are reasonable, we cannot guarantee that the future results, levels of activity, performance or events and circumstances reflected in the forward-looking statements will be achieved or occur. Except as required by law, including the securities laws of the United States, we do not intend to update any forward-looking statements to conform these statements to actual results or to changes in our expectations.
INDUSTRY AND MARKET DATA
In addition to the industry, market and competitive position data referenced in this report from our own internal estimates and research, some market data and other statistical information included in this report are based in part upon information obtained from third-party industry publications, research, surveys and studies, none of which we commissioned. Third-party industry publications, research, surveys and studies generally indicate that their information has been obtained from sources believed to be reliable, although they do not guarantee the accuracy or completeness of such information.
We are responsible for all of the disclosure in this report, and while we believe that each of the publications, research, surveys and studies included in this report are prepared by reputable sources, we have not independently verified market and industry data from third-party sources. In addition, while we believe our internal company research and estimates are reliable, such research and estimates have not been verified by independent sources. Assumptions and estimates of our and our industry’s future performance are necessarily subject to a high degree of uncertainty and risk due to a variety of factors, including those described in “Part I. Item 1A. Risk Factors.” These and other factors could cause our future performance to differ materially from our assumptions and estimates. See “Cautionary Note Regarding Forward-Looking Statements.”
PART I
|
Item 1. |
Business |
Overview
We are a clinical stage biopharmaceutical company primarily focused on the development of novel recombinant (synthetic) proteins. Our goal is to use our trade secrets, patented and licensed technologies to establish our company as a leader in the development and commercialization of therapeutic treatments derived from novel recombinant proteins. Our current focus is on chronic kidney disease (CKD) and acute ischemic stroke (AIS). We are working to advance DM199, our lead drug candidate, through required clinical trials to create shareholder value by establishing its clinical and commercial potential as a therapy for CKD and AIS.
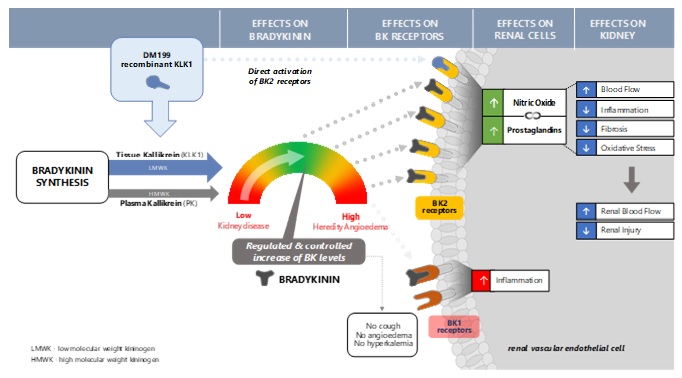
DM199 is a recombinant form of human tissue kallikrein-1 (KLK1). KLK1 is a serine protease (protein) produced primarily in the kidneys, pancreas and salivary glands that plays a critical role in the regulation of local blood flow and vasodilation (the widening of blood vessels, which decreases vascular resistance) in the body, as well as an important role in inflammation and oxidative stress (an imbalance between potentially damaging reactive oxygen species, or free radicals, and antioxidants in the body). We believe DM199 has the potential to treat a variety of diseases where healthy function requires sufficient activity of KLK1 and its system, the kallikrein-kinin system (KKS).
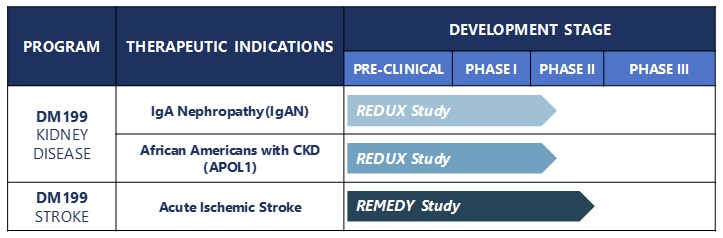
Our current product candidates in clinical development are as follows:
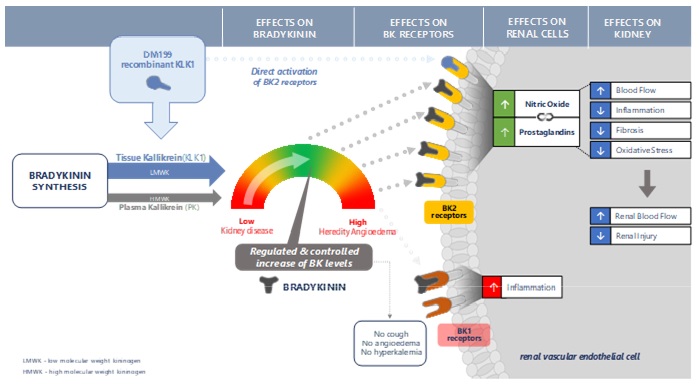
KLK1 is involved in multiple biochemical processes. The most well-characterized activity of KLK1 is enzymatic cleavage of low molecular weight kininogen (LMWK) to produce bradykinin (BK)-like peptides, collectively known as kinins, which activate BK receptors (primarily BK2R with some BK1R). Activation of BK receptors by kinins sets in motion metabolic pathways that can improve blood flow (through vasodilation), dampen inflammation, and protect tissues and end-organs from ischemic damage. Scientific literature, including publications in Circulation Research, Immunopharmacology and Kidney International, suggests that lower endogenous KLK1 levels in patients are associated with diseases related to vascular disorders, such as kidney diseases, stroke and hypertension. DM199, as a protein replacement therapy, may replenish KLK1 levels to properly activate the KKS producing nitric oxide, prostaglandin and other anti-inflammatory mediators that protect the kidney and brain from damage. By providing additional supply of KLK1 protein, DM199 treatment could potentially improve blood flow to and reduce inflammation in damaged end-organs, such as the kidneys and the brain, supporting their structural integrity and normal functioning.
DM199 (KLK1): Increasing Renal Blood Flow:
We believe DM199 may provide new treatment options with significant benefits over the current standards of care by offering potentially fewer side effects and a therapeutic treatment option to a greater number of patients. We are not aware of any approved therapies in the United States or the European Union to address low KLK1 levels and we are positioning DM199 for worldwide use. To date, clinical trials have been and/or are being conducted in the United States, Europe and Australia to support regulatory filings in the United States and around the world; with an initial focus on the United States.
In June 2019, we announced interim results from our Phase Ib study of DM199 in patients with moderate or severe CKD caused by Type I or Type II diabetes. These results, consistent with prior studies, demonstrated that DM199 continued to be safe and well tolerated with no treatment-related serious adverse events (SAEs). Pharmacokinetic (PK) data supported the determination of the dose range expected to normalize KLK1 levels in both moderate and severe CKD patients. We were also pleased to note that the PK profiles were similar between moderate and severe CKD patients, as well as previous healthy subjects, dosed at 3µg/kg. Pharmacodynamic data (PD) were also evaluated through exploratory biomarkers as pre-defined secondary endpoints for this study. Although subjects only received a single dose in the study, favorable overall results were observed approximately 24 hours after DM199 administration, including short-term improvements in Nitric Oxide (NO), average increase of 35.2%, Prostaglandin E2 (PGE2), average increase of 41.2%, eGFR, average increase of 4.08 mL/min/1732, and the urinary albumin to creatinine ratio (UACR), average decrease of 18.7%. The Company believes these observations show drug activity, consistent with the DM199 mechanism of action, and may represent initial proof-of-mechanism. Full results of the study will be provided in a peer-reviewed publication and/or poster presentation.
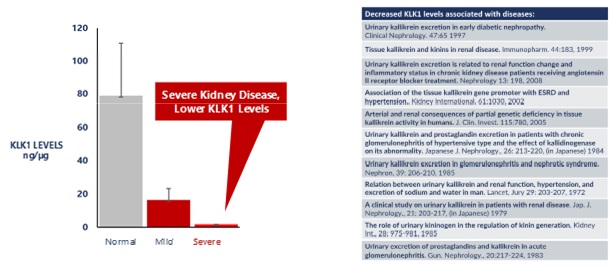
For patients with chronic kidney disease, studies have shown that KLK1 excretion, or levels of KLK1 in the urine, were significantly decreased. This decrease was more pronounced in patients with severe renal failure requiring dialysis, as illustrated in the graph below.
Low KLK1 Levels Are Associated With Chronic Kidney Disease
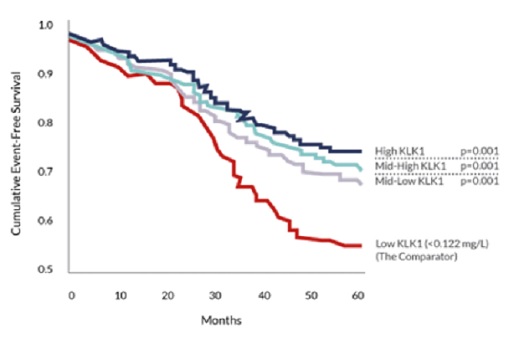
Studies have also shown that lower KLK1 levels are also a predictor of stroke recurrence. As shown in the graph below, the red line represents patients in the lowest KLK1 quartile who are at the highest risk for recurrence of stroke. (2,478 stroke patients and event free survival over 5 years).
Our Strategy
Our goal is to become a leader in the discovery, development and commercialization of recombinant proteins for the treatment of severe and life-threatening diseases. We seek to identify and select, for development and partnership, recombinant proteins with novel mechanisms that have biological properties with broad applicability. Once we have selected a class of recombinant proteins, we apply their biological properties to clinical settings with unmet needs. We evaluate opportunities based on the estimated development timeline, cost, regulatory pathway and commercial opportunity. After identifying suitable molecules for clinical development, we intend to mitigate development risk by maintaining a diversified and broad clinical pipeline, analyzing data to determine the potential of each program and entering into development collaborations with industry-leading companies.
Currently, our strategy includes the following key components:
|
● |
DM199 for CKD - complete our ongoing Phase II study |
|
● |
DM199 for AIS - complete our ongoing Phase II study |
|
● |
DM199 for other vascular diseases - initiate Phase II studies, with sufficient resources |
|
● |
Leverage our technologies to expand our development pipeline |
|
● |
Use our expertise to identify and manufacture other novel recombinant proteins |
Targeted Indications and Markets for DM199
Chronic Kidney Disease
CKD is characterized by a progressive decline in overall kidney function as measured by the glomerular filtration rate (GFR) (a test used to evaluate blood flow through the kidneys), and albuminuria (a marker for glomerular injury measuring the amount of albumin protein excreted in your urine or how well the kidneys are filtering excess fluid and waste products out of your blood). As glomerular filtration decreases, the body’s ability to continue to regulate its many functions as well as eliminate metabolic waste is lost and ultimately, may result in severe physiologic consequences. Among multiple underlying causes, CKD often begins with an increase in blood glucose, which leads to the thickening of the glomerular membrane, known as fibrosis. As the kidney function becomes impaired, GFR decreases and abnormal amounts of protein are released into the urine collecting tubules of the kidney through damaged capillary pores in the glomerular floor. Additionally, increased blood glucose leads to increased blood pressure, elevated reactive oxygen species, advanced glycation end product formation (harmful compounds that are formed when protein or fat combine with sugar in the bloodstream) and inflammation. As these continue, structural components of the kidney begin to collapse, resulting in cell ischemia and cell death. As the renal damage continues, a progressive thickening of the glomerular basement membrane is seen along with continued pathological changes in the cells and inflammation. Early stages of CKD are characterized as microalbuminuria (small amounts of protein leak into the urine). Late stages are characterized as macroalbuminuria (large amounts of protein leak into the urine). The rate of decline depends on a number of factors including the type of diabetes, genetic predisposition, glycemic controls and blood pressure. At the final stages of CKD, the kidneys fail completely and dialysis or a kidney transplant is needed.
CKD is a widespread health problem that generates significant economic burden throughout the world:
|
● |
According to the National Kidney Foundation, 30 million Americans and 120 million Chinese suffer from this debilitating and potentially life-threatening condition. |
|
● |
The primary causes of CKD are diabetes (Type 2 and Type 1) and hypertension. The Medical Clinics of North America estimates that over 40% of those with Type 2 diabetes and 20% of those with Type 1 diabetes will eventually develop CKD, making it one of the more common risks for diabetics. |
|
● |
Patients with CKD are at greater risk for hypertension and heart disease. |
Currently, there is no cure for CKD and treatment primarily involves management of the symptoms of the disease. Blood pressure medications, such as angiotensin converting enzyme inhibitors (ACEi) or angiotensin receptor blockers (ARB), are often prescribed to control hypertension, and hopefully, slow the progression of CKD. However, according to the National Kidney Foundation, many of these patients continue to show declining kidney function and 3.6% of the overall population has a lifetime risk of developing ESRD, where dialysis or a kidney transplant is needed. We believe DM199 may offer a novel approach for the treatment CKD since the KLK1 protein plays a vital role in maintaining normal kidney function. As observed in a Phase 1B clinical trial, DM199 promotes the production of nitric oxide, prostacyclin and other anti-inflammatory mediators which are critical for kidney health and integrity. Since patients with moderate to severe CKD often excrete abnormally low levels of KLK1 in their urine, DM199, by increasing levels of KLK1, may prevent or reduce further kidney damage by replenishing KLK1 levels and restoring the protective BK system.
Acute Ischemic Stroke
Stroke is characterized by the rapidly developing loss of brain function due to a blockage of blood flow in the brain. As a result, the affected area of the brain becomes inactive and eventually dies. Strokes can be classified into two major categories: AIS and hemorrhagic stroke. AIS is characterized by interruption of the blood supply by a blood clot (ischemia), while a hemorrhagic stroke results from rupture, or bleeding, of a blood vessel or an abnormal vascular structure. According to the U.S. Center for Disease Control and Prevention (CDC), about 87% of strokes are ischemic in nature with the remainder classified as hemorrhagic. According to the CDC, worldwide, stroke is an important cause of adult disability and the second leading cause of death in developed countries. Risk factors for stroke include advanced age, hypertension (high blood pressure), previous stroke or transient ischemic attack (TIA), diabetes, high cholesterol, cigarette smoking and atrial fibrillation. According to the World Health Organization, each year approximately 15 million people worldwide suffer a stroke, of which 5.5 million will die and 5.0 million will be permanently disabled. According to the CDC:
|
● |
Every year in the United States, approximately 795,000 people experience a new or recurrent stroke (ischemic or hemorrhagic). Approximately 610,000 of these are first events and 185,000 are recurrent stroke events. |
|
● |
Approximately one of every 20 deaths in the United States is caused by stroke. On average, someone in the United States has a stroke every 40 seconds and someone dies from a stroke every four minutes. |
|
● |
Stroke costs the United States an estimated $34 billion annually, including the cost of health care services, medications and lost productivity. |
More specifically, with respect to an ischemic stroke, at the site of a blood flow blockage in the brain, there exist two major ischemic zones - the core ischemic zone with nearly complete loss of blood flow (blood flow below 10% to 25%), and the surrounding ischemic penumbra, a rim of mild to moderately ischemic tissue surrounding the core ischemic zone. Within minutes, the significant lack of blood flow in the core ischemic zone (i.e., glucose and oxygen deprivation) rapidly depletes energy stores and triggers the loss of ion gradients, ultimately leading to neuronal cell death. The ischemic penumbra zone, however, may remain viable for several hours via collateral arteries that branch from the main occluded artery in the core ischemic zone. Unfortunately, the penumbra is at great risk of delayed tissue damage due to inflammation and cell death, or apoptosis. As time goes on, a lack of blood flow in the core ischemic zone (infarct) may lead to fluid buildup (edema) and swelling which creates intracranial pressure. This pressure on the brain leads to tissue compression resulting in additional ischemia. Additional events in AIS include vascular damage to the blood vessel lining or endothelium, loss of structural integrity of brain tissue and blood vessels, and inflammation. A stroke can lead to permanent damage with memory loss, speech problems, reading and comprehension difficulties, physical disabilities, and emotional/behavioral problems. The long-term costs of stroke are substantial, with many patients requiring extended hospitalization, extended physical therapy or rehabilitation, and/or long-term institutional or family care. However, provided the extended window of viability in the penumbra, next generation stroke therapies are being developed to protect valuable brain tissue during the hours to a week after a stroke.
Acute Ischemic Stroke Treatment Options
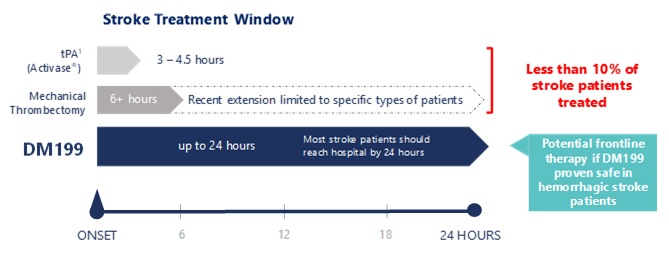
Stroke represents an area of significant unmet medical need and a KLK1 treatment (such as DM199) could provide a novel treatment option with an added significant patient benefit in that its proposed therapeutic window is up to 24 hours after the first sign of stroke symptoms. Currently, the only pharmacological intervention for AIS is tissue plasminogen activator (tPA), which must be given within 4.5 hours of symptom onset. Mechanical thrombectomy, in which the clot is removed using catheter-based tools, is also available to some patients. Despite the availability of these treatments, many patients are not eligible due to the location of the clot, the elapsed time after the occurrence of the stroke, or other safety considerations. Thus, we believe DM199 offers significant advantages over the current treatment options and fills an unmet need for patients who cannot receive tPA. Additionally, DM199 may also offer a complimentary follow-on treatment for patients who initially receive tPA or mechanical thrombectomy. Based on the number of strokes each year (approximately 1.7 million in the United States, Europe and Japan and 15 million worldwide) and considering the $8,500 estimated cost per patient for the current standard of care, tPA, we believe the annual market opportunity for DM199 could be significant.
DM199 Acute Ischemic Stroke: Proposed Mechanism
KLK1, primarily derived from human urine, is widely used in China (marketed under the brand name Kailikang®) for the treatment of AIS, making KLK1 therapy available to hundreds of thousands of Chinese patients who currently have no options. We believe that the proprietary DM199 protein could result in improved efficacy with optimized pharmacokinetics (drug level exposure) and avoid the side effects of Kailikang, specifically the risk of endotoxins, impurities and antibody formation associated with Kailikang given that it is isolated from human urine. DM199 also addresses potential supply constraints that makes Kailikang difficult and expensive to produce given the limited source of human urine. These factors make the recombinant protein DM199 a product candidate that is better positioned for regulatory approval worldwide compared to a urine-derived protein since it can meet the rigorous required manufacturing standards.
Potential Treatments with DM199
Chronic Kidney Disease
We believe DM199 has the potential to offer therapeutic benefits for CKD patients. The KLK1 protein plays a vital role in normal kidney function, promoting the production of nitric oxide, prostacyclin and other anti-inflammatory mediators which are important for kidney health and integrity. Patients with moderate to severe CKD often excrete abnormally low levels of KLK1 in their urine, leading to the hypothesis that a KLK1 deficit contributes to disease progression. We believe that DM199, as a protein replacement therapy, can replenish KLK1 levels and properly activate the KKS producing nitric oxide, prostacyclin and other anti-inflammatory mediators which may protect the kidney from damage. In fact, DM199 treatment in an animal model of Type 1 diabetes delayed the onset of the disease, attenuated the degree of insulitis (inflammation in the insulin producing islet cells of the pancreas) and improved pancreatic beta cell mass in a dose-dependent manner by increasing regulatory T cells (Tregs). By providing additional KLK1, DM199 has the potential to:
|
● |
Improve blood flow through the kidney by restoring proper regulation of blood flow through veins, arteries and especially capillaries (vasoregulation); |
|
● |
Support the structural integrity of the kidney by reducing scar tissue formation (fibrosis), oxidative stress, and inflammation; and |
|
● |
Activate mechanisms that upregulate Tregs, improve insulin sensitization, glucose uptake and glycogen synthesis, and lower blood pressure. |
Further supporting the hypothesis that an intact KKS is critical for normal kidney function, a series of observational studies published in Immunopharmacology showed the amount of KLK1 released into the urine appears to be inversely correlated with the severity of disease in patients with CKD. Urinary KLK1 excretion was decreased in patients with both mild (not requiring dialysis) and severe (kidney failure/hemodialysis) renal disease compared to controls. Decreases in urinary KLK1 activity were seen especially when the reduction was associated with decreased glomerular filtration rate.
DM199 treatment is intended to directly replenish KLK1 levels to maintain, or possibly restore, kidney function. Current treatment options, especially ACEi drugs, only partially restore kidney function and are associated with high-risk side effects. Importantly, it is becoming increasingly clear that part of the beneficial effect of ACEi drugs involves preventing the normal breakdown of BK leading to substantial increases in BK levels throughout the body. However, these effects can be unregulated and ACEi drugs therefore can generate excessive BK where is it not needed, potentially leading to side effects such as persistent cough, angioedema (swelling of skin and tissue) and hyperkalemia (abnormally high potassium levels that can lead to cardiac arrest and sudden death). We believe DM199 treatment could allow KLK1 to follow its normal physiological processes and release BK when and where it is needed, avoiding these side effects.
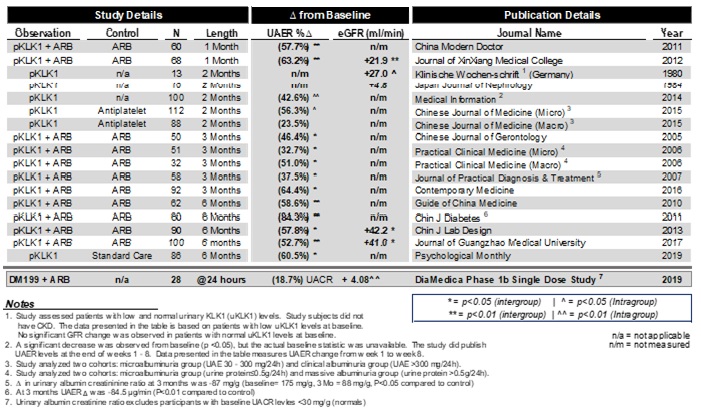
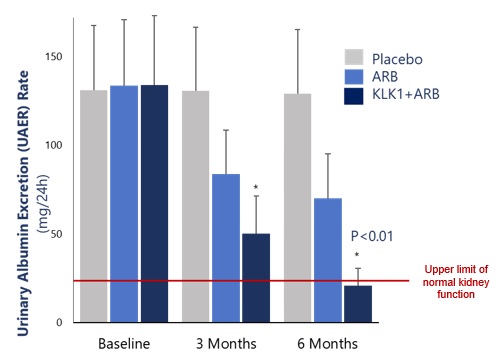
KLK1 derived from the pancreas of a pig, or porcine KLK1, is currently used to treat CKD in Japan, China and Korea. Specifically, porcine KLK1 is also used to treat hypertension and retinopathy. Based on data published by the data analytics company IQVIA and internal analysis, we estimate that millions of patients have been treated with porcine KLK1 for these and other vascular diseases in Asia. We have identified 17 clinical papers, published in China and Germany supporting the therapeutic activity of porcine KLK1 in CKD patients, whether given alone or in combination with an ARB or an ACEi. We also identified one 90-patient study in which porcine KLK1 given in combination with an ARB restored normal kidney function. These unblinded studies involve treatment durations ranging from a few weeks up to six months and report improvement in kidney disease based on decreased urinary albumin excretion rates and other clinical endpoints of kidney disease.
Kalidinogenase (Porcine-Derived KLK1) Improves Kidney
Function in 90 Patients
There is a significant need for new and alternative treatment strategies for CKD. The combined results of these studies, which are consistent with the observed movements in secondary endpoints in our Phase Ib study in CKD patients, and preclinical studies of DM199 provide rationale for the continued clinical development of DM199. We intend to seek approval for use of DM199 as a novel and ground-breaking therapy for CKD. We believe DM199 could replace an ACEi and/or complement the use of an ARB to improve kidney functions without increasing the risk of hyperkalemia, chronic cough, angioedema or other related side effects. Protein replacement therapy with DM199, through the activation of the KKS, may complement the renin-angiotensin system, primarily targeted ARBs. Activation of the KKS system may improve the function of the diseased renal system by improving blood flow and vasodilation, as well as reducing inflammation and oxidative stress. We anticipate that DM199 will boost KLK1 levels to release physiological levels of BK when and where needed, generating beneficial nitric oxide and prostacyclin while increasing Tregs to reduce inflammation.
DM199 (Recombinant KLK1) Proposed Mechanism of Actions
Acute Ischemic Stroke
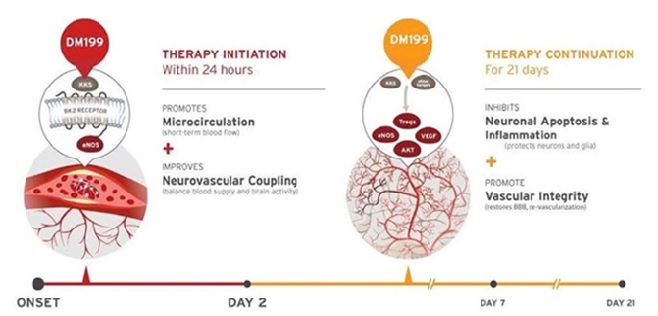
We believe treatment of AIS with DM199 could have both immediate and long-term benefits for patients that could significantly improve outcomes following AIS. Immediate actions include activation of the KKS to release nitric oxide and improve microcirculation in ischemic tissue along with improvements in the balance between blood flow and brain activity (neurovascular coupling). Long-term (days following the stroke) actions include the restoration of the blood brain barrier through increases in Tregs – a subpopulation of T cells that modulate the immune system and prevent autoimmune disease and inhibition of apoptotic cell death.
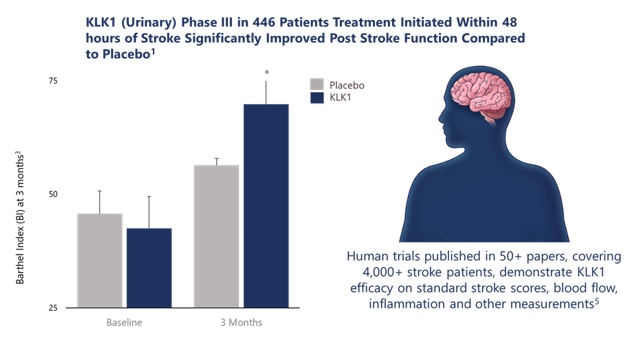
In China, Kailikang is approved and marketed by Techpool Bio-Pharma Inc., a company controlled by Shanghai Pharmaceuticals Holding Co. Ltd. We believe Kailikang has been approved for the treatment of AIS in China with a treatment window of up to 48 hours post-stroke. Based on IQVIA data, other publications and internal analysis, we estimate that over 500,000 stroke patients have been treated with Kailikang in Asia. More than 50 published clinical studies, covering over 4,000 stroke patients, have demonstrated a beneficial effect of Kailikang treatment in AIS. According to a publication in the China Journal of Neurology, in a double-blinded, placebo-controlled trial of 446 patients treated with either Kailikang or a placebo administered up to 48 hours after a stroke showed significantly better scores on the European Stroke Scale and Activities of Daily Living at three weeks post-treatment and after three months using the Barthel Index.
Furthermore, a comprehensive meta-analysis covering 24 clinical studies involving 2,433 patients published in the Journal of Evidence-Based Medicine concluded that human urinary KLK1 appears to ameliorate neurological deficits for patients with AIS and improves long-term outcomes, though a few treated patients suffered from transient hypotension.
As DM199 is a recombinant form of human KLK1, we believe it has the potential to preserve “at risk” brain tissue by increasing cerebral blood flow, establishing better collateral circulation, decreasing inflammation, reducing cell death, or apoptosis, and facilitating improved blood flow to at-risk brain tissue in the ischemic penumbra. DM199 offers the potential of an improved recombinant product for worldwide use. We are developing DM199 to treat AIS patients with a therapeutic window of up to 24 hours after the first sign of symptoms, well beyond the current window of up to 4.5 hours for tPA, thereby filling a large unmet need for patients who cannot receive tPA under the currently available treatment window of tPA. This important attribute could potentially make therapy available to the millions of patients worldwide who currently have limited treatment options.
DMDx Diagnostic Tool
Creation of a diagnostic tool, DMDx, to measure KLK1 levels in urine or plasma would support treatment with DM199 if it is approved for commercial sale. Several published studies indicate KLK1 insufficiency is associated with multiple disease states including hypertension, CKD and AIS. Levels of endogenous KLK1 in both urine and plasma are inversely correlated with disease severity. DMDx, if successfully developed, has the potential to help physicians identify patients at risk for these multiple disease states. The decision to commence this study will be dependent upon our available cash resources.
Our Competition and Current Treatments for Chronic Kidney Disease and Acute Ischemic Stroke
The biopharmaceutical industry is highly competitive and characterized by rapidly advancing technologies that focus on rapid development of proprietary drugs. We believe that our product candidates, development capabilities, experience and scientific knowledge provide us with competitive advantages. However, we face significant potential competition from many different sources, including major pharmaceutical, specialty pharmaceutical and biotechnology companies, academic institutions, governmental agencies and other research institutions. Any product candidates that we successfully develop and commercialize will compete with existing therapies and new therapies that may become available in the future.
Many of our competitors, either alone or with their strategic partners, have substantially greater financial, technical and human resources than we do, and experience in obtaining FDA and other regulatory approvals of treatments and commercializing those treatments. Accordingly, our competitors may be more successful than us in obtaining approval for competitive products and achieving widespread market acceptance. Our competitors’ treatments may be more effectively marketed and sold than any products we may commercialize, thus limiting our market share and resulting in a longer period before we can recover the expenses of developing and commercializing our product candidates.
Mergers and acquisitions in the biotechnology and pharmaceutical industries may result in even more resources being concentrated among a smaller number of our competitors. Smaller or early stage companies may also prove to be significant competitors, particularly through collaborative arrangements with large and established companies. These activities may lead to consolidated efforts that allow for more rapid development of competitive product candidates.
We also compete for staff, development and clinical resources. These competitors may impair our ability to recruit or retain qualified scientific and management personnel, our ability to work with specific advisors, or our ability to work with clinical contract organizations due to conflicts of interest or capacity constraints, and may also delay recruitment of clinical study sites and study volunteers, impeding progress in our development programs.
We expect any products that we develop and commercialize to compete on the basis of, among other things, efficacy, safety, price and the availability of reimbursement from government or other third-party payers. Our commercial opportunity could be reduced or eliminated if our competitors develop and commercialize products that are viewed as safer, more effective or less expensive than any products that we may develop.
Chronic Kidney Disease
In the United States, we are aware of only one currently approved treatment for CKD. That treatment is an ACEi (marketed under the brand name Captopril®) which is approved for the treatment of patients with CKD caused by Type 1 diabetes. There are several pharmaceutical products for the treatment of CKD currently in clinical development, some of which include:
|
● |
Mineralcorticortisteroid receptor agonist (Bayer HealthCare Pharmaceuticals LLC) |
|
● |
CCR2 receptor antagonists (ChemoCentryx, Inc., Bristol-Myers Squibb Company) |
|
● |
Oxidative stress, cyclo-oxygenase 2 inhibitors (Reata Pharmaceuticals, Inc.) |
|
● |
Glycosylation inhibitors (Glycadia, Inc. aka Glycadia Pharmaceuticals) |
|
● |
Endothelin A receptor antagonists (AbbVie Inc.) |
|
● |
Cyclin nucleotide phosphodiesterase inhibitor (Pfizer Inc.) |
|
● |
Aldosterone receptor antagonists (Mitsubishi Tanabe Pharma Corporation) |
|
● |
Nitric oxide enzyme inhibitor (GenKyoTex SA) |
|
● |
Nitric oxide (Cyclerion/Ironwood Pharmaceuticals, Inc.) |
Current treatment strategies for CKD include the strict control of high blood pressure and high blood sugar. The ACEi drug Captopril® is approved for use in patients with CKD due to Type 1 diabetes and both ACEi and ARBs are widely prescribed to slow the progression of CKD. Furthermore, the treatment with ACEi has been linked to hyperkalemia (elevated blood potassium levels), which increases the risk for abnormal heart rhythms and sudden death. In fact, two clinical trials investigating the use of ACEi and ARB combination therapy in kidney disease were stopped prematurely because participants developed hyperkalemia. The added complication of hyperkalemia results in patients receiving smaller, or suboptimal, doses or patients being untreated because they cannot tolerate the treatment. Additional side effects with ACEi treatment are angioedema (swelling of skin tissue) and persistent cough.
DM199 treatment is intended to directly replenish KLK1 levels, maintaining or potentially restoring kidney function. Current treatment options, especially ACEi drugs, only partially restore kidney function and are associated with high-risk side effects. ACEi drugs can generate excessive BK where it is not needed, potentially leading to side effects such as cough and angioedema. DM199 treatment may potentially allow KLK1 to follow its normal physiological processes and release BK when and where it is needed, avoiding these side effects.
Acute Ischemic Stroke
Currently, there is one approved pharmaceutical treatment for acute ischemic stroke. That treatment is tPA (marketed under the brand name Activase®), and its therapeutic window is limited to up to 4.5 hours after the AIS. There are, however, a number of companies that are actively pursuing a variety of approaches to develop pharmaceutical products for the treatment of AIS including, among others:
|
● |
Stem cells (Athersys, Inc.) |
|
● |
Cerebral edema (Biogen Inc.) |
|
● |
Anti-inflammatory and clot dissolving (Biogen Inc.) |
|
● |
Cell protection and anti-inflammation (ZZ Biotech LLC) |
|
● |
Inhibiting platelet aggregation (Acticor Biotech SAS) |
There is a large unmet therapeutic need for AIS treatments that can be administered beyond the 4.5-hour time window of tPA. With this large unmet therapeutic need, there is significant competition to develop new therapeutic options. New therapeutic options in development include tissue protection focused therapies (deliverable from hours to days after the stroke) that preserve and protect brain cells beyond the tPA therapeutic window. Currently, the most advanced treatments involve the mechanical removal of blood clots in brain arteries through sophisticated catheter-based approaches. According to published research, use of mechanical thrombectomy is growing and the window of time after a stroke where the procedure can be used is widening. These therapies are especially targeted toward preserving viable cells in the ischemic penumbra hours after a stroke. The goal is to provide treatment options for the vast majority of AIS patients who do not receive hospital care early enough to qualify for tPA therapy. We believe there is a very significant market opportunity for a drug that has a therapeutic window beyond that of tPA and is able to obtain regulatory approval.
In January 2019, we announced the publication of a paper titled “Human Tissue Kallikrein in the Treatment of Acute Ischemic Stroke” in the peer reviewed journal, Therapeutic Advances in Neurological Disorders. The paper reviews the scientific literature covering the biochemical role of KLK1 and presents the mechanistic rationale for using KLK1 as an additional pharmacological treatment for AIS. In addition to the biochemical mechanism of KLK1, the review highlights supporting results from human genetics and preclinical animal models of brain ischemia. It also reviews published clinical results for treatment of AIS by a form of KLK1 that is isolated from human urine. This form has been approved for post-infarct treatment of AIS in China and data has been published on clinical trials involving over 4,000 patients. The paper offers a series of testable therapeutic hypotheses for demonstrating the long-term beneficial effect of KLK1 treatment in AIS patients and the reasons for this action.
DM199 Clinical Studies
CKD Phase Ib
During 2019, DiaMedica initiated and completed a Phase Ib clinical trial of DM199 in 32 subjects with moderate or severe CKD caused by Type I or Type II diabetes mellitus. The study was performed at three sites in the U.S. and was designed to assess the pharmacokinetics (PK) of three dose levels of DM199 (3, 5 and 8 µg/kg), administered in a single subcutaneous (SC) dose, as well as the evaluation of safety, tolerability and secondary pharmacodynamic (PD) endpoints. Results from the study were also used to guide the design of Phase II CKD studies.
We announced positive interim results from the first 28 subjects. PK profiles, at the 3µg/kg dose level, were similar between moderate and severe CKD patients, and consistent with healthy subjects (normal kidney function) tested previously. Therefore, we do not believe dosing adjustment is warranted, based on the presence or severity of CKD and a full renal study will likely not be required. Final study results indicated that DM199 was observed to be well tolerated with no dose-limiting tolerability observed in the study. There were no deaths, no discontinuations due to a treatment-related adverse event (AE), and no treatment-related significant adverse events (SAEs). AEs were minor and consistent with standard treatment(s) in the CKD patient population.
Favorable overall PD interim results were also observed including short-term improvements in Nitric Oxide (NO), average increase of 35.2%, Prostaglandin E2 (PGE2), average increase of 41.2%, estimated glomerular flow rate (eGFR), average increase of 4.08 mL/min/1732, and the UACR, excluding subjects with normal UACR levels, average decrease of 18.7%. PD results appeared to be drug related in that greatest improvements occurred at approximately 24 hours after DM199 administration and subsequently declined.
CKD Phase II REDUX Study
In October 2019, the FDA accepted our Phase II clinical trial protocol for the treatment of CKD caused by rare or significant unmet diseases. The trial named REDUX, Latin for restore, is a multi-center, open-label investigation of approximately 60 participants with CKD, who are being enrolled in two cohorts (30 participants per cohort). The study is being conducted in the United States at up to 12 sites and is focused on participants with two specific causes of CKD. Cohort I is focused on non-diabetic, hypertensive African Americans with Stage II or III CKD. African Americans are at greater risk for CKD than Caucasians, and those who have the APOL1 gene mutation are at an even higher risk. The study is designed to capture the APOL1 gene mutation as an exploratory biomarker in this cohort. Cohort II is focused on participants with IgA Nephropathy (IgAN). The study will evaluate two dose levels of DM199 within each cohort. Study participants will receive DM199 by subcutaneous injection twice weekly for 95 days. The primary study endpoints include safety, tolerability, blood pressure, albuminuria and kidney function, which will be evaluated by changes from baseline in eGFR and albuminuria, as measured by the UACR. Participant enrollment and dosing for this study commenced in December 2019.
AIS Phase II REMEDY Study
In February 2018, treatment was initiated for the first patient in our Phase II REMEDY trial assessing the safety, tolerability and markers of therapeutic efficacy of DM199 in patients suffering from AIS. Our REMEDY trial was expected to enroll up to 100 patients to evaluate DM199 in patients with AIS. The study drug (DM199 or placebo) was administered as an intravenous (IV) infusion within 24 hours of stroke symptom onset, followed by SC injections later that day and once every 3 days for 21 days. The study was designed to measure safety and tolerability along with multiple tests designed to investigate DM199’s therapeutic potential including plasma-based biomarkers and standard functional stroke measures assessed at 90 days post-stroke. Standard functional stroke measurements include the Modified Rankin Scale, National Institutes of Health Stroke Scale, the Barthel Index and C-reactive protein, a measure of inflammation.
In October 2019, we completed enrollment in the REMEDY trial. Final enrollment was 92 participants.
Other Clinical Studies
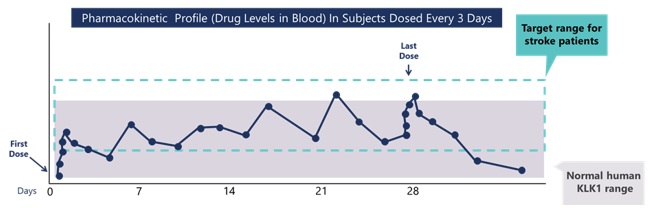
In 2017, we completed and published, in the International Journal of Clinical Trials, results from, a Phase Ib study with DM199 designed to assess the safety, tolerability, pharmacokinetics, and pharmacodynamics in healthy volunteers. This study compared multiple dose levels of DM199, administered via IV and SC routes to identify a dose and delivery route that most closely compared to or improved upon the pharmacokinetic and pharmacodynamics profile of the approved urinary KLK1 in China. We found that a dose of DM199 administered via IV infusion mimicked the drug profile of IV-administered urinary derived KLK1 (Kailikang). This study also identified a dose of DM199, administered via SC injection, which had a superior pharmacokinetic profile and that maintained more normal KLK1 levels throughout the day. Below are results from our clinical trial showing the pharmacokinetic profile of subcutaneously administered DM199 observed in study subjects as compared to what we believe is normal range in healthy subjects.
During 2013 and 2014, five clinical trials were completed with DM199 in over 120 volunteers, including multiple Phase I single dose ascending and multiple dose ascending studies in healthy volunteers and patients with Type 2 diabetes. Chronic dosing studies over 16 to 28 days were also conducted in healthy volunteers and patients with Type 2 diabetes (see below). As is generally the case for early phase clinical trials, the primary endpoints for all studies were safety, tolerability, and pharmacokinetics. The Phase II (Part D) study also investigated a series of secondary endpoints that included blood glucose concentration, insulin levels, glucose tolerance testing and a variety of experimental biomarkers evaluating the potential efficacy of DM199 in treating Type 2 diabetes patients.
DM199 Trial Design Overview
|
Trial |
Participants (N) |
Design |
Doses (µg/kg) |
Route |
Length |
|
Phase-I Part A |
Healthy (32) |
Single ascending dose |
5, 15, 30, 50 |
SC |
1 week |
|
Phase-I Part B |
Type 2 diabetes (10) |
Single ascending dose |
0.3, 1.5, 15 |
SC |
1 week |
|
Phase-I Part C |
Healthy (18) |
Multiple ascending dose |
3, 15, 25 |
SC |
6 doses over 16 days |
|
Phase-IIA Part D |
Type 2 diabetes (36) |
Blinded multiple dose |
Placebo, 3, 15 |
SC |
10 doses over 28 days |
|
Phase I Bridging |
Healthy (36) |
Single ascending dose |
0.25, 0.50, 0.75 1.0 3.0 |
IV IV SC |
1 week |
In combination, these studies showed that DM199 was well tolerated and demonstrated clear physiological activity. After SC injection, DM199 exhibited a favorable pharmacokinetic profile with extended half-life (i.e., the time required to reduce concentration of the drug in the body by one-half), supporting potential dosing intervals of up to one week. The dose-limiting tolerability issue in healthy volunteers was orthostatic hypotension (a condition in which blood pressure falls significantly when a person stands) observed largely at the 50 µg/kg dose level, which is much greater than the dose level anticipated to be efficacious in patients. In each trial, observed treatment emergent side-effects were mild to moderate in severity and resolved. The most common treatment-emergent side effects included headache, dizziness, nausea and injection site pain, the majority of which were observed in the highest dose group of the Phase I-Part A trial.
Two of these clinical studies focused on patients with Type 2 diabetes. The first study enrolled 10 Type 2 diabetic patients. The patients were dosed with either DM199, at three single ascending dose levels or placebo. DM199 was well-tolerated at all three dose levels by the diabetic patients with no dose limiting side effects. The second study in patients with Type 2 diabetes enrolled 36 patients treated with one of two SC dose levels of DM199 or placebo over 28 days. This study achieved its primary endpoints and demonstrated that DM199 was well-tolerated. The secondary endpoints for this study, however, were not met. The secondary efficacy endpoints were confounded due to what we believe were significant execution errors caused by protocol deviations occurring at the clinical trial site that were unable to be reconciled. See “Part I. Item 1. Business—Legal Proceedings” for more information on this study.
Potential DM199 Commercial Advantages
Several researchers have studied the structural and functional properties of KLK1. This deep body of knowledge has revealed the potential clinical benefits of KLK1 treatments. Today, forms of KLK1 derived from human urine and porcine pancreas are sold in Japan, China and Korea to treat acute ischemic stroke, chronic kidney disease, retinopathy, hypertension and related diseases. We are not aware of any synthetic version of KLK1 with regulatory approval for human use in any country, nor any synthetic version in development besides our drug candidate DM199 (recombinant human KLK1). We believe at least five companies have attempted, unsuccessfully, to create a synthetic version of KLK1.
The growing understanding of the role of KLK1 in human health and its use in Asia as an approved therapeutic highlight two important potential commercial advantages for DM199:
|
● |
KLK1 treatment is sold in Japan, China and Korea. Research has shown that low levels of KLK1 are associated with patients suffering from a variety of diseases related to vascular dysfunction, such as chronic kidney disease, acute ischemic strokes, retinopathy and hypertension. Clinical trial data with human urine and porcine pancreas derived KLK1 treatments have demonstrated statistically significant clinical benefits from the treatment of a variety of patients with KLK1 compared to placebo. These efficacy results are further substantiated by established markets in Japan, China and Korea for pharmaceutical sales of KLK1 derived from human urine and porcine pancreas. |
|
● |
KLK1 treatment has had limited side effects and has been well tolerated in studies to date. KLK1 is naturally produced by the human body; and therefore, the body’s own control mechanisms act to limit potential side effects. The only notable side effect observed in our clinical trials was orthostatic hypotension, or sudden drop in blood pressure, which was primarily seen at doses significantly higher than our anticipated therapeutic dose levels. Routine clinical use of KLK1 treatment in Asia has been well-tolerated by patients. In 2017, we completed a clinical trial comparing the pharmacokinetic profile of DM199 to Kailikang for acute ischemic stroke, which showed DM199, when administered in intravenous form, to have a profile similar to Kailikang. Further, when DM199 was administered subcutaneously, DM199 demonstrated a superior, longer acting, pharmacokinetic profile than Kailikang. |
We have conducted numerous internal and third-party analyses to demonstrate that DM199 is structurally and functionally equivalent to KLK1 derived from human urine. The amino acid structure of DM199 is identical to the human urine form, and the enzymatic and pharmacokinetic profiles are substantially similar to both human urine and porcine derived KLK1. The physiological effects of DM199 on blood pressure, from our completed studies, mirror that of human urine and porcine-derived forms of KLK1. We believe that the results of this work suggest that the therapeutic action of DM199 will be the same or, potentially, better than that of the forms marketed in Asia. In addition, we believe that there are also significant formulation, manufacturing, regulatory and other advantages for synthetic human KLK1 drug candidate DM199:
|
● |
Potency and Impurity Considerations. KLK1 derived from human urine or porcine pancreas may contain impurities, endotoxins and chemical byproducts due to the inherent variability of the isolation and purification process. This creates the risk of inconsistencies in potency and impurities from one production run to the next. However, we expect to produce a consistent formulation of KLK1 that is free of endotoxins and other impurities. |
|
● |
Cost and Scalability. Large quantities of human urine and porcine pancreas must be obtained to derive a small amount of KLK1. This creates potential procurement, cost and logistical challenges to source the necessary raw organic material, particularly for human urine sourced KLK1. Once sourced, the raw organic material is processed using chemicals and costly capital equipment and produces a significant amount of byproduct waste. Our novel recombinant manufacturing process utilizes widely available raw materials and can be readily scaled for commercial production. Accordingly, we believe our manufacturing process has significant cost and scalability advantages. |
|
● |
Regulatory. We are not aware of any attempts by manufacturers of the urine or porcine based KLK1 products to pursue regulatory approvals in the United States. It is theorized that this is related to challenges presented by using inconsistent and potentially hazardous biomaterials, such as human urine and porcine pancreas, and their resulting ability to produce a consistent drug product. Our novel recombinant manufacturing process utilizes widely available raw materials which we believe provides a significant regulatory advantage, particularly in regions such as the United States, Europe and Canada, where safety standards are high. In addition, DM199 could qualify for 12 years of data exclusivity under the Biologics Price Competition and Innovation Act of 2009, which was enacted as part of the Patient Protection and Affordable Care Act, as amended by the Health Care and Education Reconciliation Act of 2010 (collectively, the ACA). |
Regulatory Approval
Securing regulatory approval for the manufacture and sale of human therapeutic products in the United States, Europe, Canada and other commercial territories is a long and costly process that is controlled by that particular territory’s national regulatory agency. The national regulatory agency in the United States is the FDA, in Europe it is the European Medicines Agency (EMA), and in Canada it is Health Canada. Other national regulatory agencies have similar regulatory approval processes, but each national regulatory agency has its own approval processes. Approval in the United States, Europe or Canada does not assure approval by other national regulatory agencies, although often test results from one country may be used in applications for regulatory approval in another country.
Prior to obtaining regulatory approval to market a drug product, every national regulatory agency has a variety of statutes and regulations which govern the principal development activities. These laws require controlled research and testing of products, governmental review, and approval of a submission containing preclinical and clinical data establishing the safety and efficacy of the product for each use sought, approval of manufacturing facilities including adherence to good manufacturing practices (GMP) during production and storage, and control of marketing activities, including advertising, labeling and pricing approval.
None of our product candidates have been completely developed or tested; and, therefore, we are not yet in a position to seek regulatory approval in any territory to market any of our product candidates.
The clinical testing, manufacturing, labeling, storage, distribution, record keeping, advertising, promotion, import, export, and marketing, among other things, of our product candidates are subject to extensive regulation by governmental authorities in the United States and other countries. The process of obtaining regulatory approvals and the subsequent compliance with appropriate federal, state, local, and foreign statutes and regulations require the expenditure of substantial time and financial resources. Failure to comply with the applicable requirements at any time during the product development process, approval process, or after approval may subject us to a variety of administrative or judicial sanctions, including refusal by the applicable regulatory authority to approve pending applications, withdrawal of an approval, imposition of a clinical hold, issuance of warning letters and other types of letters, product recalls, product seizures, total or partial suspension of production or distribution, injunctions, fines, refusals of government contracts, restitution, disgorgement of profits, or civil or criminal investigations and penalties brought by the FDA and the Department of Justice or other governmental entities.
U.S. Approval Process
In the United States, the FDA is responsible for the drug approval process. The FDA’s mission is to ensure that all medications on the market are safe and effective. The FDA’s approval process examines and thoroughly reviews potential new drugs; only those that are in compliance with the Code of Regulations, 21 CFR 312 and 21 CFR 314 are approved.
The U.S. food and drug regulations require licensing of manufacturing facilities, carefully controlled research and testing of products, governmental review and approval of test results prior to marketing of therapeutic products, and adherence to GMP, as defined by each licensing jurisdiction, during production.
A description of the different stages in the drug approval process in the United States follows.
Stage 1: Preclinical Research. After an experimental drug is discovered, research is conducted to help determine its potential for treating or curing an illness. This is called preclinical research. Animal and/or bench studies are conducted to determine if there are any harmful effects of the drug and to help understand how the drug works. Information from these experiments is submitted to the FDA as part of an investigational new drug (IND) application. The FDA reviews the information in the IND and decides if the drug is safe to study in humans.
Stage 2: Clinical Research. The experimental drug is studied in humans. The studies are known as clinical trials. Clinical trials are carefully designed and controlled experiments in which the experimental drug is administered to patients to test its safety and to determine the effectiveness of an experimental drug. The four general phases of clinical research are described below.
|
● |
Phase I Clinical Studies. Phase I clinical studies are generally conducted with healthy volunteers who are not taking other medicines; patients with the illness that the drug is intended to treat are not tested at this stage. Ultimately, Phase I studies demonstrate how an experimental drug affects the body of a healthy individual. Phase I consists of a series of small studies consisting of “tens” of volunteers. Tests are done on each volunteer throughout the study to see how the person’s body processes, responds to, and is affected by the drug. Low doses and high doses of the drug are usually studied, resulting in the determination of the safe dosage range in volunteers by the end of Phase I. This information will determine whether the drug proceeds to Phase II. |
|
● |
Phase II Clinical Studies. Phase II clinical studies are conducted in order to determine how an experimental drug affects people who have the disease to be treated. Phase II usually consists of a limited number of studies that help determine the drug’s short-term safety, side effects, and general effectiveness. The studies in Phase II often are controlled investigations involving comparison between the experimental drug and a placebo, or between the experimental drug and an existing drug. Information gathered in Phase II studies will determine whether the drug proceeds to Phase III. |
|
● |
Phase III Clinical Studies. Phase III clinical studies are expanded controlled and uncontrolled trials that are used to more fully investigate the safety and effectiveness of the drug. These trials differ from Phase II trials because a larger number of patients are studied (sometimes in the thousands) and because the studies are usually double blinded, placebo controlled and of longer duration. As well, Phase III studies can include patients who have more than one illness and are taking medications in addition to the experimental drug used in the study. Therefore, the patients in Phase III studies more closely reflect the general population. The information from Phase III forms the basis for most of the drug’s initial labeling, which will guide physicians on how to use the drug. |
|
● |
Phase IV Clinical Studies. Phase IV clinical studies are conducted after a drug is approved. Phase IV studies may be required by the FDA or conducted by companies to more fully understand how their drug compares to other drugs. FDA-required Phase IV studies often investigate the drug in specific types of patients that may not have been included in the Phase III studies and can involve very large numbers of patients to further assess the drug’s safety. |
Stage 3: FDA Review for Approval. Following the completion of Phase III clinical studies, the pharmaceutical company prepares an electronic common technical document reporting all clinical nonclinical and chemistry, manufacturing and control studies conducted on the drug that is transmitted to the FDA as a New Drug Application (NDA). The FDA reviews the information in the NDA to determine if the drug is safe and effective for its intended use. An advisory panel meeting is scheduled for a new drug allowing the FDA to gain feedback from experts. If the FDA determines that the drug is safe and effective, the drug will be approved.
Stage 4: Marketing. After the FDA has approved the experimental drug, the pharmaceutical company can make it available to physicians and their patients. A company also may continue to conduct research to discover new uses for the drug. Each time a new use for a drug is discovered, the drug once again is subject to the entire FDA approval process before it can be marketed for that purpose.
Any FDA approved pharmaceutical products are subject to continuing regulation by the FDA, including, among other things, record-keeping requirements, reporting of adverse experiences with the product, providing the FDA with updated safety and efficacy information, product sampling and distribution requirements, complying with certain electronic records and signature requirements and complying with FDA promotion and advertising requirements, which include, among others, standards for direct-to-consumer advertising, promoting pharmaceutical products for uses or in patient populations that are not described in the pharmaceutical product’s approved labeling (known as “off-label use”), industry-sponsored scientific and educational activities and promotional activities involving the internet. Failure to comply with FDA requirements is likely to have negative consequences, including adverse publicity, enforcement letters from the FDA, mandated corrective advertising or communications with doctors, and civil or criminal penalties.
The FDA also may require post-marketing testing, known as Phase IV testing, risk evaluation and mitigation strategies and surveillance to monitor the effects of an approved product or place conditions on an approval that could restrict the distribution or use of the product.
DM199 may qualify for 12 years of data exclusivity under the Biologics Price Competition and Innovation Act of 2009 (the BPCIA), which was enacted as part of the ACA. Under the BPCIA, an application for a biosimilar product (BLA) cannot be submitted to the FDA until four years, or if approved by the FDA, until 12 years, after the original brand product identified as the reference product is approved under a BLA. The BPCIA provides an abbreviated pathway for the approval of biosimilar and interchangeable biological products. The new abbreviated regulatory pathway establishes legal authority for the FDA to review and approve biosimilar biologics, including the possible designation of a biosimilar as “interchangeable” based on its similarity to an existing brand product. The new law is complex and is only beginning to be interpreted and implemented by the FDA.
European Approval Process
The EMA is roughly parallel to the U.S. FDA in terms of the drug approval process and the strict requirements for approval. The EMA was set up in 1995 in an attempt to harmonize, but not replace, the work of existing national medicine regulatory bodies in individual European countries. As with the FDA, the EMA drug review and approval process follows similar stages from preclinical testing through clinical testing in Phase I, II, and III. There are some differences between the FDA and EMA review process, specifically the review process in individual European countries. Such differences may allow certain drug products to be tested in patients at an earlier stage of development.
Other Healthcare Laws and Compliance Requirements
In the United States, our activities are potentially subject to regulation by various federal, state and local authorities in addition to the FDA, including the Centers for Medicare and Medicaid Services and other divisions of the U.S. government, including, the Department of Health and Human Services, the U.S. Department of Justice and individual U.S. Attorney offices within the Department of Justice, and state and local governments. For example, if a drug product is reimbursed by Medicare, Medicaid, or other federal or state healthcare programs, our company, including our sales, marketing and scientific/educational grant programs, must comply with the federal False Claims Act, as amended, the federal Anti-Kickback Statute, as amended, and similar state laws. If a drug product is reimbursed by Medicare or Medicaid, pricing and rebate programs must comply with, as applicable, the Medicaid rebate requirements of the Omnibus Budget Reconciliation Act of 1990 (OBRA), and the Medicare Prescription Drug Improvement and Modernization Act of 2003. Among other things, OBRA requires drug manufacturers to pay rebates on prescription drugs to state Medicaid programs and empowers states to negotiate rebates on pharmaceutical prices, which may result in prices for our future products being lower than the prices we might otherwise obtain. Additionally, the ACA substantially changes the way healthcare is financed by both governmental and private insurers. There may continue to be additional proposals relating to the reform of the U.S. healthcare system, in the future, some of which could further limit coverage and reimbursement of drug products. If drug products are made available to authorized users of the Federal Supply Schedule of the General Services Administration, additional laws and requirements may apply.
Pharmaceutical Coverage, Pricing and Reimbursement
In the United States and markets in other countries, sales of any products for which we receive regulatory approval for commercial sale will depend in part on the availability of coverage and adequate reimbursement from third-party payers, including government health administrative authorities, managed care providers, private health insurers and other organizations. In the United States, private health insurers and other third-party payers often provide reimbursement for products and services based on the level at which the government (through the Medicare and/or Medicaid programs) provides reimbursement for such treatments. Third-party payers are increasingly examining the medical necessity and cost-effectiveness of medical products and services in addition to their safety and efficacy; and, accordingly, significant uncertainty exists regarding the coverage and reimbursement status of newly approved therapeutics. In particular, in the United States, the European Union and other potentially significant markets for our product candidates, government authorities and third-party payers are increasingly attempting to limit or regulate the price of medical products and services, particularly for new and innovative products and therapies, which has resulted in lower average selling prices. Further, the increased emphasis on managed healthcare in the United States and on country and regional pricing and reimbursement controls in the European Union will put additional pressure on product pricing, reimbursement and usage, which may adversely affect our future product sales and results of operations. These pressures can arise from rules and practices of managed care groups, judicial decisions and governmental laws and regulations related to Medicare, Medicaid and healthcare reform, pharmaceutical reimbursement policies and pricing in general. As a result, coverage and adequate third party reimbursement may not be available for our products to enable us to realize an appropriate return on our investment in research and product development.
The market for our product candidates for which we may receive regulatory approval will depend significantly on access to third-party payers’ drug formularies or lists of medications for which third-party payers provide coverage and reimbursement. The industry competition to be included in such formularies often leads to downward pricing pressures on pharmaceutical companies. Also, third-party payers may refuse to include a particular branded drug in their formularies or may otherwise restrict patient access to a branded drug when a less costly generic equivalent or another alternative is available. In addition, because each third-party payer individually approves coverage and reimbursement levels, obtaining coverage and adequate reimbursement is a time-consuming and costly process. We would be required to provide scientific and clinical support for the use of any product candidate to each third-party payer separately with no assurance that approval would be obtained, and we may need to conduct expensive pharmacoeconomic studies to demonstrate the cost-effectiveness of our product candidates. This process could delay the market acceptance of any of our product candidates for which we may receive approval and could have a negative effect on our future revenues and operating results. We cannot be certain that our product candidates will be considered cost-effective. If we are unable to obtain coverage and adequate payment levels for our product candidates from third-party payers, physicians may limit how much or under what circumstances they will prescribe or administer them and patients may decline to purchase them. This in turn could affect our ability to successfully commercialize our products and impact our profitability, results of operations, financial condition, and future success.
Research and Development
We have devoted substantially all of our efforts to research and development (R&D) which therefore comprises the largest component of our operating costs. Our primary focus over the past approximately eight years has been our lead product candidate, DM199, which is currently in clinical development for the treatment of CKD and AIS.
We expect our R&D expenses will continue to increase in the future as we advance our initial product candidate, DM199, through clinical trials in CKD and AIS and seek to expand our product candidate portfolio. The process of conducting the necessary clinical research to obtain regulatory approval is costly and time-consuming and we consider the active management and development of our clinical pipeline to be integral to our long-term success. The actual probability of success for each product candidate, clinical indication and preclinical program may be affected by a variety of factors including, among other things, the safety and efficacy data for each product candidate, amounts invested in their respective programs, competition and competitive developments, manufacturing capability and commercial viability.
Research and development expenses include:
|
● |
expenses incurred under contract research agreements and other agreements with third parties; |
|
● |
expenses incurred under agreements with clinical trial sites that conduct research and development activities on our behalf; |
|
● |
employee and consultant-related expenses, which include salaries, benefits, travel and share-based compensation; |
|
● |
laboratory and vendor expenses related to the execution of clinical trials and non-clinical studies; |
|
● |
the cost of acquiring, developing, manufacturing, and distributing clinical trial materials; and |
|
● |
facilities and other expenses, which include direct and allocated expenses for rent and maintenance of facilities, insurance, and other supply costs. |
Research and development costs are expensed as incurred. Costs for certain development activities such as clinical trials are recognized based on an evaluation of the progress to completion of specific tasks using information and data provided to us by our vendors and our clinical sites.
We expect that it will be several years, if ever, before we have any product candidates ready for commercialization.
Manufacturing
We do not own or operate manufacturing facilities for the production of clinical or commercial quantities of DM199 nor do we have plans to develop our own manufacturing operations in the foreseeable future. We rely on Catalent Pharma Solutions, LLC (Catalent) for all of our required raw materials, active pharmaceutical ingredients and finished DM199 product candidate for our clinical trials. We have licensed certain gene expression technology and we contract with Catalent for the manufacture of DM199. The royalty term is indefinite but the license agreement may be canceled by us on 90 days’ prior written notice. The license may not be terminated by Catalent unless we fail to make required milestone and royalty payments. We currently employ internal resources and third-party consultants to manage our manufacturing relationship with Catalent.
Sales and Marketing
We have not yet defined our sales, marketing or product distribution strategy for our initial product candidate, DM199, or any future product candidates, because it is still early in the clinical development stage. We currently expect to partner with a large pharmaceutical company for sales execution. However, our future commercial strategy may include the use of distributors, a contract sales force or the establishment of our own commercial and specialty sales force, as well as similar strategies for regions and territories outside the United States.
Intellectual Property
We view patents and other means of intellectual property protection including trade secrets as an important component of our core business. We focus on translating our innovations into intangible property protecting our proprietary technology from infringement by competitors. To that end, patents are reviewed frequently and continue to be sought in relation to those components or concepts of our preclinical and clinical products to provide protection. Our strategy, where possible, is to file patent applications to protect our product candidates, as well as methods of manufacturing, administering and using a product candidate. Prior art searches of both patent and scientific databases are performed to evaluate novelty, inventiveness and freedom-to-operate. We require all employees, consultants and parties to a collaborative research agreement to execute confidentiality agreements upon the commencement of employment, consulting relationships or a collaboration with us. These agreements require that all confidential information developed or made known during the course of the engagement with us is to be kept confidential. We also maintain agreements with our scientific staff and all parties contracted in a scientific capacity affirming that all inventions resulting from work performed for us, using our property or relating to our business and conceived or completed during the period covered by the agreement are the exclusive property of DiaMedica.
Our DM199 patent portfolio includes three granted U.S. patents, a granted European patent and pending applications in Australia, Canada, China, Europe, India, Japan, Korea and the United States. Granted or pending claims offer various forms of protection for DM199 including claims to compositions of matter, pharmaceutical compositions, specific formulations and dosing levels and methods for treating a variety of diseases, including chronic kidney disease, stroke and related disorders. These U.S. patents and applications, and their foreign equivalents, are described in more detail below.
Issued patents held by us cover the DM199 composition of matter based on an optimized combination of closely-related isoforms that differ in the extent of glycosylation (process by which sugars are chemically attached to proteins). Issued claims in this patent family cover the most pharmacologically active variants of DM199 and methods of using the same for treating ischemic conditions and these patents are due to expire in 2033. A second patent family includes an issued U.S. patent with claims directed to methods of treating subjects by administering a SC formulation of DM199 or related recombinant kallikrein-1 polypeptides and is predicted to expire in 2033. The pending applications are directed to a range of dose levels and dosing regimens of DM199 that are potentially useful for treating a wide range of diseases including, e.g. pulmonary arterial hypertension, cardiac ischemia, chronic kidney disease, diabetes, stroke and vascular dementia which, if granted, are predicted to expire in 2038.
We do not own or operate manufacturing facilities for the production of clinical or commercial quantities of DM199. We are contracting with Catalent, a contract manufacturing organization (CMO) with proven GMP experience in the manufacturing of recombinant proteins for clinical trials, for the manufacture of DM199. We have licensed certain gene expression technology and we contract with Catalent for the manufacture of DM199. Under the terms of this license, certain milestone and royalty payments may become due and are dependent upon, among other factors, performing clinical trials, obtaining regulatory approvals and ultimately the successful commercialization of a new drug, the outcome and timing of which is uncertain. The royalty term is indefinite but the license agreement may be canceled by us on 90 days’ prior written notice. The license may not be terminated by Catalent unless we fail to make required milestone and royalty payments.
Methods and reagents required for commercial scale manufacture of DM199 are subject to a series of patents issued to Catalent. As noted above, we exclusively license these patents from Catalent for the production of DM199 or any human KLK1 protein.
We believe that our proprietary technology along with trade secrets and specialized knowledge of the manufacturing process will provide substantial protection from third-party competitors. We also believe that DM199 cannot be easily reverse engineered for the production of a copycat version.
We believe that the most relevant granted patents and applications with composition of matter or method of use claims covering DM199 are listed below, along with their projected expiration dates exclusive of any patent term extension:
|
Patent/Application Number |
Title |
Geography |
Predicted Expiration |
|||
|
Issued patents |
||||||
|
US 9,364,521 |
Human Tissue Kallikrein 1 Glycosylation Isoforms |
US |
2033 |
|||
|
US 9,839,678 |
Human Tissue Kallikrein 1 Glycosylation Isoforms |
US |
2033 |
|||
|
EP 2 854 841 |
Human Tissue Kallikrein 1 Glycosylation Isoforms |
Europe |
2033 |
|||
|
US 9,616,015 |
Formulations for Human Tissue Kallikrein-1 for Parenteral Delivery and Related Methods |
US |
2033 |
|||
|
Pending applications |
||||||
|
AU 2018230478 |
Dosage Forms of Tissue Kallikrein 1 |
Australia |
2038 |
|||
|
CA 3054962 |
Dosage Forms of Tissue Kallikrein 1 |
Canada |
2038 |
|||
|
CN 201880016380.4 |
Dosage Forms of Tissue Kallikrein 1 |
China |
2038 |
|||
|
EP 18763243.5 |
Dosage Forms of Tissue Kallikrein 1 |
Europe |
2038 |
|||
|
IN 201917037712 |
Dosage Forms of Tissue Kallikrein 1 |
India |
2038 |
|||
|
JP 2019-548655 |
Dosage Forms of Tissue Kallikrein 1 |
Japan |
2038 |
|||
|
KR 10-2019-7026369 |
Dosage Forms of Tissue Kallikrein 1 |
Korea |
2038 |
|||
|
US 16/492,059 |
Dosage Forms of Tissue Kallikrein 1 |
US |
2038 |
In September 2018, we entered into a license and collaboration agreement with Ahon Pharmaceutical Co Ltd. (Ahon Pharma), which granted Ahon Pharma exclusive rights to develop and commercialize DM199 for acute ischemic stroke in mainland China, Taiwan, Hong Kong S.A.R. and Macau S.A.R. Under the terms of the agreement, we received an upfront payment of $500,000 on signing and were entitled to receive an additional payment of $4.5 million upon the earlier of July 1, 2019 or regulatory clearance to initiate a clinical trial in China. On August 12, 2019, after extensive good faith discussions between Ahon Pharma and the Company, the parties were unable to agree upon mutually acceptable revised terms to the agreement and DiaMedica terminated this license agreement due to Ahon Pharma’s non-payment of the milestone due on July 1, 2019. As a result of this termination, DiaMedica regained worldwide rights for DM199 for acute ischemic stroke.
Employees
As of December 31, 2019, we had 8 full-time employees and 1 part-time employee. We have never had a work stoppage and none of our employees are covered by collective bargaining agreements. We believe our employee relations are good.
Information About Our Executive Officers
The following table sets forth information as of December 31, 2019 regarding each of our current executive officers:
|
Name |
Age |
Positions |
||
|
Rick Pauls |
48 |
President and Chief Executive Officer, Director |
||
|
Scott Kellen |
54 |
Chief Financial Officer and Secretary |
||
|
Harry Alcorn, Pharm.D. |
63 |
Chief Medical Officer |
||
|
Sydney Gilman, Ph.D. |
67 |
Vice President, Regulatory Affairs |
The present principal occupations and recent employment history of each of our executive officers are set forth below.
Rick Pauls was appointed our President and Chief Executive Officer in January 2010. Mr. Pauls has served as a member of our Board of Directors since April 2005 and the Chairman of the Board from April 2008 to July 2014. Prior to joining DiaMedica, Mr. Pauls was the Co-Founder and Managing Director of CentreStone Ventures Inc., a life sciences venture capital fund, from February 2002 until January 2010. Mr. Pauls was an analyst for Centara Corporation, another early stage venture capital fund, from January 2000 until January 2002. From June 1997 until November 1999, Mr. Pauls worked for General Motors Acceptation Corporation specializing in asset-backed securitization and structured finance. Mr. Pauls previously served as an independent member of the board of directors of LED Medical Diagnostics, Inc. Mr. Pauls received his Bachelor of Arts in Economics from the University of Manitoba and his M.B.A. in Finance from the University of North Dakota.
Scott Kellen was appointed our Chief Financial Officer and Secretary in April 2018. Prior to joining DiaMedica, Mr. Kellen served as Vice President and Chief Financial Officer of Sun BioPharma, Inc., a publicly-traded clinical stage drug development company, from October 2015 until April 2018. From February 2010 to September 2015, Mr. Kellen served as Chief Financial Officer and Secretary of Kips Bay Medical, Inc., a publicly-traded medical device company, and became Chief Operating Officer of Kips Bay in March 2012. From November 2007 to May 2009, Mr. Kellen served as Finance Director of Transoma Medical, Inc. From 2005 to October 2007, Mr. Kellen served as Corporate Controller of ev3 Inc. From March 2003 to April 2005, Mr. Kellen served as Senior Manager, Audit and Advisory Services of Deloitte & Touche, LLP. Altogether, Mr. Kellen has spent more than 25 years in the life sciences industry, focusing on publicly traded early stage and growth companies. Mr. Kellen has a Bachelor of Science degree in Business Administration from the University of South Dakota and is a Certified Public Accountant (inactive).
Harry Alcorn Jr. Pharm.D. was appointed our Chief Medical Officer in August 2018. Prior to joining DiaMedica, Dr. Alcorn served as Chief Scientific Officer at DaVita Clinical Research (DCR), a company that provides clinical research services for Pharmaceutical and Biotech companies, from October 1997 to June 2018. While at DCR, Dr. Alcorn was responsible for clinical research operations, including the formation and management of the early clinical and late phase research services. Dr. Alcorn also founded the U.S. Renal Network, the first network of Phase I renal research sites in the United States. Dr. Alcorn developed DCR’s site management organization for clinical trials. Dr. Alcorn also served as an Executive Director, a Pharmacist and an Investigator at DCR. During this time, from January 2013 to December 2014, he also served on the Board of Directors for the Association of Clinical Pharmacology Units, an association of Phase I clinical trial sites. Dr. Alcorn has over 30 years of clinical research experience working with biotech and pharmaceutical companies, both public and private, in conducting research in renal, hepatic and cardiovascular disease. Dr. Alcorn has written and consulted on the development of several protocols and has served as Principal Investigator or Sub Investigator in numerous studies and, for several of these studies, presented study design and results to the FDA. Currently he holds clinical faculty appointments with the University of Minnesota, Creighton University, University of Nebraska Medical Center, Virginia Commonwealth and the University of Colorado, Denver. Dr. Alcorn graduated from Creighton University with a Bachelor of Pharmacy and went on to earn his Doctor of Pharmacy degree from University of Nebraska Medical Center.
Sydney A. Gilman, Ph.D. was appointed our Vice President, Regulatory Affairs effective as of November 1, 2019. Dr. Gilman is currently the founder and President of Trident Rx Consulting Services LLC, a regulatory consulting firm, a position he has held since January 2004. Dr. Gilman is a former U.S. Food and Drug Administration (FDA) Chemistry reviewer. He spent six years at the FDA in various CDER Therapeutic Drug Divisions of the Center for Drug Evaluation and Research with consulting ties to both Biologics and Devices. Dr. Gilman also has an additional 20 years of experience in the pharmaceutical industry in positions ranging from Senior Scientist to Director to Vice President Responsibilities. He earned his Bachelor of Science from Loyola College and a Ph.D. in Organic Chemistry from the University of Pittsburgh.
Enforceability of Civil Liabilities Against Foreign Persons
We are corporation governed under British Columbia’s Business Corporations Act (BCBCA). There is doubt as to the enforceability, in original actions in Canadian courts, of liabilities based upon the U.S. federal securities laws or the securities laws or “blue sky” laws of any state within the United States and as to the enforceability in Canadian courts of judgments of U.S. courts obtained in actions based upon the civil liability provisions of the U.S. federal securities laws or any such state securities laws or blue sky laws. Accordingly, it may not be possible to enforce judgments obtained in the United States against us.
Available Information
We are a corporation governed under the BCBCA. Our company was initially incorporated under the name Diabex Inc. pursuant to The Corporations Act (Manitoba) by articles of incorporation dated January 21, 2000. Our articles were amended (i) on February 26, 2001 to change our corporate name to DiaMedica Inc., (ii) on April 11, 2016 to continue the Company from The Corporations Act (Manitoba) to the Canada Business Corporations Act (CBCA), (iii) on December 28, 2016 to change our corporate name to DiaMedica Therapeutics Inc., (iv) on September 24, 2018 to permit us to hold shareholder meetings in the United States and to permit our directors, between annual meetings of our shareholders, to appoint one or more additional directors to serve until the next annual meeting of shareholders; provided, however, that the number of additional directors shall not at any time exceed one-third of the number of directors who held office at the expiration of the last meeting of shareholders, (v) on November 15, 2018 to effect a 1-for-20 consolidation of our common shares, and (vi) on May 31, 2019, to continue our existence from a corporation incorporated under the CBCA into British Columbia under the BCBCA.
Our registered office is located at 301-1665 Ellis Street, Kelowna, British Columbia, V1Y 2B3 and our principal executive office is located at our wholly owned subsidiary, DiaMedica USA Inc., located at Two Carlson Parkway, Suite 260, Minneapolis, Minnesota, USA 55447. Our telephone number is 763-496-5454. Our internet website address is http://www.diamedica.com. Information contained on our website does not constitute part of this report.
We make available, free of charge and through our Internet web site, our annual reports on Form 10-K, quarterly reports on Form 10-Q, current reports on Form 8-K, and any amendments to any such reports filed or furnished pursuant to Section 13(a) or 15(d) of the Securities Exchange Act of 1934, as amended, as soon as reasonably practicable after we electronically file such material with, or furnish it to, the Securities and Exchange Commission (SEC). Reports filed with the SEC may be viewed at www.sec.gov.
Implications of Being an Emerging Growth Company
We are an emerging growth company as defined in the Jumpstart Our Business Startups Act of 2012 (JOBS Act), and we may remain an emerging growth company for up to five years from December 31, 2018. However, if certain events occur prior to the end of such five-year period, including if we become a large accelerated filer, our annual gross revenue exceeds $1.07 billion, or we issue more than $1.0 billion of non-convertible debt in any three-year period, we will cease to be an emerging growth company prior to the end of such five-year period. For so long as we remain an emerging growth company, we are permitted and intend to rely on exemptions from certain disclosure and other requirements that are applicable to other public companies that are not emerging growth companies. In particular, in this report, we have provided only two years of audited financial statements and have not included certain other information that would be required if we were not an emerging growth company. Accordingly, the information contained herein may be different than the information you receive from other public companies in which you hold equity interests. However, we have irrevocably elected not to avail ourselves of the extended transition period for complying with new or revised accounting standards, and, therefore, we are subject to the same new or revised accounting standards as other public companies that are not emerging growth companies.
|
Item 1A. |
Risk Factors |
The following are the most significant factors known to us that could materially adversely affect our business, operating results or financial condition.
Risks Related to Our Financial Position and Need for Additional Capital
We have incurred substantial losses since our inception and expect to continue to incur future substantial losses and may never become profitable.
We are a clinical stage biopharmaceutical company focused on the development of novel recombinant proteins. Investment in biopharmaceutical product development is highly speculative because it entails substantial upfront capital expenditures and significant risk that a product candidate will fail to prove effective, gain regulatory approval or become commercially viable. We do not have any products approved by regulatory authorities and have not generated any revenues from product sales to date, and do not expect to generate any revenue from the sale of products for several years. We have incurred significant research, development and other expenses related to our ongoing operations and expect to continue to incur such expenses. As a result, we have not been profitable and have incurred significant operating losses in every reporting period since our inception. For the years ended December 31, 2019 and 2018, we incurred a net loss of $10.6 million and $5.7 million, respectively. As of December 31, 2019, we had an accumulated deficit of $56.6 million. Our prior losses, combined with expected future losses, have had and will continue to have an adverse effect on our shareholders’ equity and working capital. We expect to continue to incur substantial operating losses as we continue our research and development (R&D) activities, planned clinical trials, regulatory activities and otherwise develop our product candidate, DM199, or any future product candidates to a point where they may be commercially sold and we begin to recognize future product sales, or receive royalty payments, licensing fees, and/or milestone payments sufficient to generate revenues to fund our continuing operations. We expect our operating losses to increase in the near term as we continue the research, development and clinical trials of, and seek regulatory approval for, our product candidates. We are unable to predict the extent of any future losses or when we will become profitable, if ever. Our failure to become and remain profitable may depress the market price of our common shares and could impair our ability to raise capital, develop products, expand our business and product offerings or continue our operations. Even if we do achieve profitability, we may not be able to sustain or increase profitability on an ongoing basis.
We currently have no revenue from product sales and do not expect any revenue from product sales for several years. Accordingly, we will need additional funding to continue our research and development activities and other operations, which may not be available to us on acceptable terms, or at all.
Our future operations will be dependent upon our ability to develop our product candidates, obtain research grant funding, obtain required regulatory approvals, generate revenue from product sales, negotiate collaboration or license agreements or other strategic alternatives, and/or secure additional funding. As of December 31, 2019, we had cash, cash equivalents and marketable securities of $7.9 million. Although we recently raised $7.7 million in net proceeds from our February 2020 public offering, we still expect we will need substantial additional capital to further our R&D activities, planned clinical trials and regulatory activities and to otherwise develop our product candidate, DM199, or any future product candidates to a point where they may be commercially sold. While we are striving to achieve these plans, there is no assurance we will be successful or that additional financing will be obtained on favorable terms or at all in furtherance of our strategic objectives. Our ability to continue as a going concern is dependent on our ability to continue obtaining sufficient funds to conduct our R&D activities and to successfully commercialize our product candidates.
We will require additional funds to finance our operations, which may not be available to us on acceptable terms, or at all. As a result, we may not complete the development and commercialization of our current DM199 product candidate or develop any new product candidates.
We require significant additional funds for further R&D activities, planned clinical trials and the regulatory approval process. We expect our current cash resources of $7.9 million in cash, cash equivalents and marketable securities as of December 31, 2019, together with the $7.7 million in net proceeds from our February 2020 public offering, to be sufficient to allow us to complete our current ongoing Phase II REMEDY trial in patients with AIS and the first two cohorts in the Phase II study in patients with CKD and to otherwise fund our planned operations through 2021. However, the amount and timing of future funding requirements will depend on many factors, including, among others:
|
● |
the rate of progress in the development of and the conduct of clinical trials with respect to our DM199 product candidate and any other future product candidates; |
|
● |
the timing and results of our ongoing development efforts, including in particular our current Phase II clinical studies; |
|
● |
the costs of our development efforts, including the conduct of clinical trials with respect to our DM199 product candidate and any other future product candidates; |
|
● |
the costs associated with identifying additional product candidates and the potential expansion of our current development programs or potential new development programs; |
|
● |
the costs to initiate and continue research, preclinical, and clinical development efforts for any future product candidates; |
|
● |
the costs necessary to obtain regulatory approvals for our DM199 product candidate and any other future product candidates; |
|
● |
the costs associated with being a public company; |
|
● |
the costs we incur in the filing, prosecution, maintenance and defense of our intellectual property; and |
|
● |
the costs related to general and administrative (G&A) support. |
We may require significant additional funds earlier than we currently expect, and there is no assurance that we will not need or seek additional funding prior to such time. We may elect to raise additional funds even before we need them if market conditions for raising additional capital are favorable.
Since our inception, we have financed our operations primarily from public and private sales of equity securities, the exercise of warrants and stock options, interest income on funds available for investment, and government grants and tax incentives, and we expect to continue this practice for the foreseeable future. We do not have any existing credit facilities under which we could borrow funds. We may seek to raise additional funds through various sources, such as equity and debt financings, or through strategic collaborations and license agreements. We can give no assurances that we will be able to secure additional sources of funds to support our operations, or if such funds are available to us, that such additional financing will be sufficient to meet our needs or on terms acceptable to us. This is particularly true if our clinical data is not positive or economic and market conditions deteriorate.
Although we have previously been successful in obtaining financing through our equity securities offerings, there can be no assurance that we will be able to do so in the future. To the extent we raise additional capital through the sale of equity or convertible debt securities, the ownership interests of our shareholders will be diluted. Debt financing, if available, may involve agreements that include conversion discounts or covenants limiting or restricting our ability to take specific actions, such as incurring additional debt, making capital expenditures or declaring dividends. If we raise additional funds through government or other third-party funding, marketing and distribution arrangements or other collaborations, or strategic alliances or licensing arrangements with third parties, we may have to relinquish valuable rights to our technologies, future revenue streams, research programs or product candidates or grant licenses on terms that may not be favorable to us. It is possible that financing will not be available or, if available, may not be on favorable terms. The availability of financing will be affected by the results of our clinical studies and other scientific and clinical research; our ability to attain regulatory approvals; market acceptance of our product candidates; the state of the capital markets generally with particular reference to pharmaceutical, biotechnology, and medical companies; the status of strategic alliance agreements; and other relevant commercial considerations. If adequate funding is not available, we may be required to implement cost reduction strategies; delay, reduce, or eliminate one or more of our product development programs; relinquish significant rights to product candidates or obtain funds on less favorable terms than we would otherwise accept; and/or divest assets or cease operations through a merger, sale, or liquidation of our company.
We are exposed to financial risk related to the fluctuation of foreign currency exchange rates and the degrees of volatility of those rates.
We may be adversely affected by foreign currency exchange rate fluctuations. To date, we have been primarily funded through issuances of equity and proceeds from the exercise of warrants and stock options, which are denominated both in U.S. and Canadian dollars. Currently, the majority of our expenditures are in U.S. dollars. However, significant costs are also incurred in Canadian dollars, British pounds, and Australian dollars; and, therefore, we are subject to foreign currency exchange rate fluctuations which may, from time to time, impact our financial position and results of operations.
Risks Related to Our Business and Our Industry
We are an early stage company with no approved products and no revenue from commercialization of any products.
We are at an early stage of development of our product candidate, DM199, for the treatment of CKD and AIS. We have not completed the development of any product candidate and, accordingly, have not begun to commercialize any product candidate or generate any revenues from any product sales. DM199 requires significant additional clinical testing and investment prior to seeking marketing approval. A commitment of substantial resources by ourselves and any potential partners to continue to conduct clinical trials for DM199 will be required to meet applicable regulatory standards, obtain required regulatory approvals, and successfully commercialize this product candidate. DM199 is not expected to be commercially available for several years, if at all.
Our prospects depend on the success of our product candidate, DM199, which is at an early stage of development, and we may not generate revenue from product sales for several years, if at all, from this product candidate or any future product candidates.
We are highly dependent on the success of DM199, and we may not be able to successfully obtain regulatory or marketing approval for, or successfully commercialize, this product candidate. To date, we have expended significant time, resources and effort on the development of DM199, including conducting preclinical and clinical trials, for the treatment of CKD and AIS. Although we intend to study the use of DM199 to treat multiple diseases, we have no other product candidates in our current clinical development pipeline. Our ability to generate revenue from product sales and to achieve commercial success in the near term will initially depend almost entirely on our ability to successfully develop, obtain regulatory approval for and then successfully commercialize DM199. Prior to commercialization of any potential product, significant additional investments will be necessary to complete the development of DM199 or any future product candidates. Preclinical and clinical trial work must be completed before DM199 or any future product candidate could be ready for use within the markets that we have identified. We may fail to develop any products, obtain regulatory approvals, complete required clinical trials successfully, or commercialize any products. Competitors may develop alternative products and methodologies to diagnose and treat the disease indications we are pursuing, thus reducing our competitive advantages. We do not know whether any of our product development efforts will prove to be effective, meet applicable regulatory standards, obtain the requisite regulatory approvals, be capable of being manufactured at a reasonable cost, or be successfully marketed. The product candidate we are currently developing is not expected to be commercially viable for several years. In addition, although no significant adverse events have occurred to date, DM199 may cause undesirable side effects. Results of early preclinical and clinical research may not be indicative of the results that will be obtained in later stages of clinical research. If regulatory authorities do not approve DM199 for the treatment of CKD and/or AIS or any future product candidates, or if we fail to maintain regulatory compliance, we will have limited ability to commercialize DM199 or any future product candidates, and our business and results of operations would be harmed. If we do succeed in developing viable products from DM199 or any future product candidates, we will face many potential obstacles, such as the need to develop or obtain manufacturing, sales and marketing, and distribution capabilities.
The clinical and commercial success of our DM199 product candidate will depend on a number of factors, many of which are beyond our control.
The clinical and commercial success of our DM199 product candidate will depend on a number of factors, many of which are beyond our control, including, among others:
|
● |
the timely initiation, continuation, and completion of our currently ongoing Phase II and future clinical trials for DM199, which will depend substantially upon requirements for such trials imposed by the FDA and other regulatory agencies and bodies; |
|
● |
our ability to demonstrate the safety and efficacy of DM199 to the satisfaction of the relevant regulatory authorities; |
|
● |
whether we are required by the FDA or other regulatory authorities to conduct additional clinical trials, and the scope and nature of such clinical trials, prior to approval to market our DM199 product candidate; |
|
● |
the timely receipt of necessary marketing approvals from the FDA and foreign regulatory authorities, including pricing and reimbursement determinations; |
|
● |
the ability to successfully commercialize our DM199 product candidate for marketing and sale, if approved by the FDA or foreign regulatory authorities, whether alone or in collaboration with others; |
|
● |
our ability and the ability of third-party manufacturers to manufacture the quantities of our DM199 product candidate with quality attributes necessary to meet regulatory requirements and at a scale and yield sufficient to meet anticipated demand at a cost that allows us to achieve profitability; |
|
● |
our success in educating health care providers and patients about the benefits, risks, administration, and use of our DM199 product candidate, if approved; |
|
● |
acceptance of our DM199 product candidate, if approved, as safe and effective by patients and the healthcare community; |
|
● |
the achievement and maintenance of compliance with all regulatory requirements applicable to our DM199 product candidate, our third-party manufacturers, and our internal operations; |
|
● |
the maintenance of an acceptable safety profile of our products, if any, following any approval; |
|
● |
the availability, perceived advantages, relative cost, relative safety, and relative efficacy of alternative and competitive treatments; |
|
● |
our ability to provide approved product with a convenient and patient-friendly administration procedure; |
|
● |
our ability to successfully enforce our intellectual property rights for our DM199 product candidate and against the products of potential competitors; and |
|
● |
our ability to avoid or succeed in third-party patent interference or patent infringement claims. |
No assurance can be provided that we will ever be able to achieve profitability through the sale of, or royalties from, our DM199 product candidate. If we or any future collaborators are not successful in obtaining approval for and commercializing our DM199 product candidate, or are delayed in completing those efforts, our business and operations would be adversely affected.
We rely and will continue to rely on third parties to plan, conduct, and monitor our preclinical and clinical trials, and their failure to perform as required could cause substantial harm to our business.
We rely and will continue to rely on third parties to conduct a significant portion of our preclinical and clinical development activities. Preclinical activities include in vivo studies in specific disease models, pharmacology and toxicology studies, and assay development. Clinical development activities include trial design, regulatory submissions, clinical patient recruitment, clinical trial monitoring, clinical data management and analysis, safety monitoring, and project management. If there is any dispute or disruption in our relationship with third parties, or if they are unable to provide quality services in a timely manner and at a feasible cost, our active development programs may face delays. Further, if any of these third parties fails to perform as we expect or if their work fails to meet regulatory requirements, our testing could be delayed, cancelled, or rendered ineffective.
We rely on a contract manufacturer over whom we have limited control. If we are subject to quality, cost, or delivery issues with the materials supplied by this or future contract manufacturers, our business operations could suffer significant harm.
Completion of our clinical trials and commercialization of our DM199 product candidate and any future product candidates require access to, or development of, facilities to manufacture our product candidates at sufficient yields and at commercial scale. Our clinical trials must be conducted with product candidates produced under applicable current good manufacturing practices (cGMP) regulations. Failure to comply with these regulations may require us to repeat clinical trials, which would delay the regulatory approval process. We rely on CMOs for manufacturing, filling, packaging, storing, and shipping DM199 in compliance cGMP regulations applicable to DM199. The FDA ensures the quality of drug products by carefully monitoring drug manufacturers’ compliance with cGMP regulations. The cGMP regulations for drugs contain minimum requirements for the methods, facilities, and controls used in the manufacturing, processing, and packing of a drug product.
We have no direct experience in manufacturing or managing third parties in manufacturing our DM199 product candidate in the volumes that are expected to be necessary to support our clinical trials and commercialization, if DM199 is approved. Our efforts to establish these capabilities may not meet our requirements as to scale-up, timeliness, yield, cost, or quality in compliance with cGMP regulations applicable to DM199. We, any future collaborators, or our experienced third-party manufacturers may encounter difficulties in production, which may include the following, among others:
|
● |
costs and challenges associated with scale-up and attaining sufficient manufacturing yields; |
|
● |
supply chain issues, including the timely availability and shelf life requirements of raw materials and supplies and the lack of redundant and backup suppliers; |
|
● |
quality control and assurance; |
|
● |
shortages of qualified personnel and capital required to manufacture large quantities of our product candidate; |
|
● |
competing capacity needs at CMOs supporting product development as quantities for supply increase; |
|
● |
establishment of commercial supply capacity through binding supply agreements; |
|
● |
compliance with regulatory requirements that vary in each country where a product might be sold; |
|
● |
capacity limitations and scheduling availability in contracted facilities; and |
|
● |
natural disasters, cyberattacks, or other force majeure events that affect facilities and possibly limit production or loss of product inventory maintained in third party storage facilities. |
There can be no assurances that our current CMOs or any future CMOs will be able to meet our timetable and requirements for our DM199 product candidate or any future product candidates. If we are unable to arrange for alternative third-party manufacturing sources on commercially reasonable terms or in a timely manner, we may be delayed in the development of DM199 and any future product candidates. Further, CMOs must operate in compliance with cGMP regulations, and failure to do so could result in, among other things, the disruption of product supplies. Our dependence upon our current CMOs and any future third parties for the manufacture of our product candidates may adversely affect our ability to develop our product candidates on a timely and competitive basis and, if we are able to commercialize our product candidates, may adversely affect our revenues from product sales and profit margins.
If clinical trials of our product candidates fail to demonstrate safety and efficacy to the satisfaction of regulatory authorities or do not otherwise produce positive results, we would incur additional costs or experience delays in completing, or ultimately be unable to complete, the development and commercialization of our product candidates.
Before obtaining marketing approval from regulatory authorities for the sale of our product candidates, we must conduct preclinical studies and extensive clinical trials in humans to demonstrate the safety and efficacy of our product candidates. Clinical testing is expensive and difficult to design and implement, can take many years to complete, and has uncertain outcomes. The outcome of preclinical studies and early clinical trials may not predict the success of later clinical trials, and interim results of a clinical trial do not necessarily predict final results. A number of companies in the pharmaceutical and biotechnology industries have suffered significant setbacks in advanced clinical trials due to lack of efficacy or unacceptable safety profiles, notwithstanding promising results in earlier trials. We do not know whether the clinical trials we are currently conducting or may conduct in the future will demonstrate adequate efficacy and safety to result in regulatory approval to market DM199 or any future product candidates in any jurisdiction. A product candidate may fail for safety or efficacy reasons at any stage of the testing process. In addition, the patient populations in our clinical studies for DM199 often have many co-morbidities that may cause severe illness or death, which may be attributed to DM199 in a manner that negatively affects the safety profile of our DM199 product candidate. If the results of our ongoing or future clinical trials for DM199 are inconclusive with respect to efficacy, if we do not meet our clinical endpoints with statistical significance, or if there are unanticipated safety concerns or adverse events that emerge during clinical trials, we may be prevented from or delayed in obtaining marketing approval, and even if we obtain marketing approval, any sales may suffer. A major risk we face is the possibility that neither our current DM199 product candidate nor any future product candidates will successfully gain market approval from the FDA or other regulatory authorities, resulting in us being unable to derive any commercial revenue from them after investing significant amounts of capital in multiple stages of preclinical and clinical testing.
If we experience delays in clinical testing, we will be delayed in commercializing our product candidates, and our business may be substantially harmed.
We cannot predict whether any clinical trials will begin as planned, will need to be restructured, or will be completed on schedule, or at all. Our product development costs will increase if we experience delays in clinical testing. Significant clinical trial delays could shorten any periods during which we may have the exclusive right to commercialize our product candidates or allow our competitors to bring products to market before us, which would impair our ability to successfully commercialize our product candidates and may harm our financial condition, results of operations and prospects. The commencement and completion of clinical trials for our product candidates may be delayed for a number of reasons, including among others:
|
● |
failure by regulatory authorities to grant permission to proceed or placing the clinical trial on hold; |
|
● |
patients failing to enroll or remain in our trials at the rates and within the timelines we expect; |
|
● |
suspension or termination of clinical trials by regulators for many reasons, including concerns about patient safety or failure of our contract manufacturers to comply with cGMP requirements; |
|
● |
any changes to our manufacturing process that may be necessary or desired; |
|
● |
delays or failure to obtain clinical supply from contract manufacturers of our product candidates necessary to conduct clinical trials; |
|
● |
product candidates demonstrating a lack of safety or efficacy during clinical trials; |
|
● |
patients choosing an alternative treatment for the indications for which we are developing any of our product candidates or participating in competing clinical trials; |
|
● |
patients failing to complete clinical trials due to dissatisfaction with the treatment, side effects, or other reasons; |
|
● |
reports of clinical testing on similar technologies and products raising safety and/or efficacy concerns; |
|
● |
competing clinical trials and scheduling conflicts with participating clinicians; |
|
● |
clinical investigators not performing our clinical trials on their anticipated schedule, dropping out of a trial, or employing methods not consistent with the clinical trial protocol, regulatory requirements or other third parties not performing data collection and analysis in a timely or accurate manner; |
|
● |
failure of our contract research organizations (CROs) to satisfy their contractual duties or meet expected deadlines; |
|
● |
inspections of clinical trial sites by regulatory authorities, Institutional Review Boards (IRBs) or ethics committees finding regulatory violations that require us to undertake corrective action, resulting in suspension or termination of one or more sites or the imposition of a clinical hold on the entire study; |
|
● |
one or more IRBs or ethics committees rejecting, suspending or terminating the study at an investigational site, precluding enrollment of additional subjects, or withdrawing its approval of the trial; |
|
● |
failure to reach agreement on acceptable terms with prospective clinical trial sites; or |
|
● |
public health crises, epidemics and pandemics, such as the novel strain of coronavirus (COVID: 19) that recently originated in China, which has already adversely impacted and may continue to adversely impact our ability to recruit or enroll subjects for our clinical trials. |
We are currently experiencing slower than expected enrollment in our Phase II studies for CKD. If this slow enrollment continues, the completion of these studies will take longer than expected.
Our product development costs will increase if we experience delays in testing or approval or if we need to perform more or larger clinical trials than planned. Additionally, changes in regulatory requirements and policies may occur, and we may need to amend study protocols to reflect these changes. Amendments may require us to resubmit our study protocols to regulatory authorities or IRBs or ethics committees for re-examination, which may impact the cost, timing or successful completion of that trial. Delays or increased product development costs may have a material adverse effect on our business, financial condition, and prospects.
Even if we complete the necessary preclinical studies and clinical trials, the regulatory approval process is expensive, time-consuming and uncertain and may prevent us or any future collaborators from obtaining approvals for the commercialization of some or all of our product candidates. As a result, we cannot predict when or if, and in which territories, we, or any future collaborators, will obtain marketing approval to commercialize a product candidate.
The process of obtaining marketing approvals, both in the United States and abroad, is expensive and may take many years, if approval is obtained at all, and can vary substantially based upon a variety of factors, including the type, complexity and novelty of the product candidates involved.
Our current product candidate and the activities associated with its development and commercialization, including design, research, testing, manufacture, safety, efficacy, quality control, recordkeeping, labeling, packaging, storage, approval, advertising, promotion, sale, distribution, import, export, and reporting of safety and other post-market information, are subject to comprehensive regulation by the FDA, the EMA and other similar foreign regulatory agencies. Failure to obtain marketing approval for a product candidate will prevent us from commercializing the product candidate. We have only limited experience in filing and supporting the applications necessary to gain marketing approvals and expect to rely on third-parties to assist us in this process. Securing marketing approval requires the submission of extensive preclinical and clinical data and supporting information to regulatory authorities for each therapeutic indication to establish the product candidate’s safety and efficacy. Securing marketing approval also requires the submission of information about the product manufacturing process to, and inspection of manufacturing facilities by, the regulatory authorities. The FDA, EMA or other regulatory authorities may determine that our product candidates may not be effective, may be only moderately effective or may prove to have undesirable or unintended side effects, toxicities or other characteristics that may preclude our obtaining marketing approval or prevent or limit commercial use. As a result, any marketing approval we ultimately obtain may be limited or subject to restrictions or post-approval commitments that render the approved product not commercially viable.
In addition, changes in marketing approval policies during the development period, changes in or the enactment of additional statutes or regulations, or changes in regulatory review for each submitted product application, may cause delays in the approval or rejection of an application. Regulatory authorities have substantial discretion in the approval process and may refuse to accept any application or may decide that our data is insufficient for approval and require additional preclinical, clinical or other studies. In addition, varying interpretations of the data obtained from preclinical and clinical testing could delay, limit or prevent marketing approval of a product candidate.
We are in litigation against Pharmaceutical Research Associates Group B.V., a contract research organization, seeking to compel them to comply with the terms of a clinical trial research agreement and their failure to perform as required could adversely affect our ability to obtain regulatory approval for DM199.
In March 2013, we entered into a clinical research agreement with Pharmaceutical Research Associates Group B.V. (PRA Netherlands) to perform a double-blinded, placebo-controlled, single-dose and multiple-dose study to evaluate the safety, tolerability, pharmacokinetics, pharmacodynamics and proof of concept of DM199 in healthy subjects and in patients with Type 2 diabetes mellitus. In one arm of this study, we enrolled 36 patients with Type 2 diabetes who were treated with two subcutaneous dose levels of DM199 over a 28-day period. This study achieved its primary endpoint and demonstrated that DM199 was well tolerated. The secondary endpoints for this study, however, were not met. We believe there were significant execution errors in Part D of the study that were caused by protocol deviations occurring at the clinical trial site that were unable to be reconciled. We believe these included dosing errors and sample mix-ups. These errors undermined our ability to interpret the secondary endpoints. To date, we have been unable to obtain the complete study records from PRA Netherlands for the arm of the study that included 36 patients with Type 2 diabetes and was intended to measure primary endpoints (safety, tolerability) and secondary endpoints (blood glucose concentration, insulin levels, glucose tolerance test and a variety of experimental biomarkers). Without these records and given our inability to reconcile the protocol deviations, we have been unable to generate a final study report. Due in part to these confounded secondary endpoints, we are not currently continuing the clinical study of DM199 for Type 2 diabetes. We have initiated litigation against PRA Netherlands to compel them to comply with the terms of the clinical research agreement, including providing full study records, and to recover damages. Litigation distracts the attention of our management from our business, is expensive and the outcome is uncertain.
Though we have entered into a litigation funding agreement to help cover the costs associated with our litigation against PRA Netherlands, there is no assurance that we will generate any recovery from the litigation and, because of the terms of the litigation funding agreement, a significant portion, if not all, of any recovery we may obtain may be due to the funder under the agreement.
On December 27, 2019, we entered into a litigation funding agreement with LEGALIST FUND II, L.P. (the Funder) for the purpose of funding our currently pending lawsuit against PRA Netherlands. Our management believes, but cannot guarantee, that this litigation funding agreement will allow us to pursue this litigation more effectively. Although the Funder made its evaluation as to the likelihood of success, litigation is very uncertain, and no assurance can be provided that, just because we have obtained litigation funding, we will be successful or that any recovery we may obtain will be significant.
Under the terms of the litigation funding agreement, the Funder agreed to pay up to an aggregate of $1.0 million to fund reasonable legal fees, court costs, and other expenses incurred by us in connection with the litigation, including $200,000 for fees and costs previously paid by us. These payments, however, are conditioned upon the transfer of venue of the litigation from Delaware to Minnesota (Transfer) and if the venue is not transferred we will not be entitled to receive any payments under the litigation funding agreement. If the venue is transferred, we agreed to repay the Funder from any proceeds arising from the litigation (Claim Proceeds) the amount of costs actually paid or otherwise funded by the Funder in connection with the litigation, plus the reimbursement of $10,000 for its diligence and underwriting costs. Additionally, we agreed to pay the Funder from the Claim Proceeds the greater of: (i) $1.0 million if repayment occurs within nine months of the Transfer, $2.0 million if repayment occurs more than nine months after the Transfer but before trial has begun, or $3.0 million thereafter; or (ii) 20% of the Claim Proceeds. In the event the Funder has not been repaid 3½ years after the Transfer, the Funder is entitled to receive interest on the unpaid amounts equal to 20% per annum commencing on the 3½ year anniversary of the Transfer. Our obligation under the litigation funding agreement to make the foregoing payments to the Funder is non-recourse and limited only to the Claim Proceeds. As a result of the agreement, if we obtain Claim Proceeds, it is possible, depending on the amount of the Claim Proceeds, that we will receive no net recovery after all payments have been made to the Funder.
We may not be able to obtain FDA acceptance of INDs to commence future clinical trials in the United States on the timelines we expect, and even if we are able to, the FDA may not permit us to proceed in a timely manner, or at all.
Prior to commencing clinical trials in the United States for future trials of our current DM199 product candidate or any trials of future product candidates, we will be required to have an accepted IND for each product candidate and for each targeted indication. During 2019, we filed and the FDA accepted an IND for the Phase Ib study and the first two cohorts in the Phase II study in patients with CKD. A submission of an IND may not result in the FDA allowing further clinical trials to begin and, once begun, issues may arise that will require us to suspend or terminate such clinical trials. Additionally, even if relevant regulatory authorities agree with the design and implementation of the clinical trials set forth in an IND, these regulatory authorities may change their requirements in the future. Failure to submit or obtain acceptance of INDs may cause the development of our product candidates to be delayed or terminated, which could materially and adversely affect our business and prospects.
If we have difficulty enrolling patients in clinical trials, the completion of the trials may be delayed or not completed at all.
As DM199 and any future product candidates advance to clinical testing, and then through progressively larger and more complex clinical trials, we will need to enroll an increasing number of patients that meet our eligibility criteria. There is significant competition for recruiting patients in clinical trials and we may be unable to enroll the patients we need to complete clinical trials on a timely basis or at all. The factors that affect our ability to enroll patients are largely uncontrollable and include, among others:
|
● |
size and nature of the patient population; |
|
● |
eligibility and exclusion criteria for the trial; |
|
● |
design of the study protocol; |
|
● |
competition with other companies for clinical sites or patients; |
|
● |
the perceived risks and benefits of the product candidate under study; |
|
● |
real or perceived availability of alternative treatments; |
|
● |
the patient referral practices of physicians; |
|
● |
the number, availability, location, and accessibility of clinical trial sites; |
|
● |
the efforts of our physician investigators and clinical trial sites to facilitate enrollment in our clinical trials; and |
| ● | public health crises, epidemics and pandemics, such as the novel strain of coronavirus (COVID: 19), which has already adversely impacted and may continue to adversely impact our ability to recruit or enroll subjects for our clinical trials. |
We are currently experiencing slower than expected enrollment in our Phase II studies for CKD. If this slow enrollment continues, the completion of these studies will take longer than expected. We may not be able to successfully initiate or continue clinical trials if we cannot timely enroll a sufficient number of eligible patients to participate in the clinical trials required by regulatory agencies. If we have difficulty enrolling a sufficient number of patients to conduct our clinical trials as planned, we may need to delay, limit, or terminate on-going or planned clinical trials, any of which could have a material adverse effect on our business and prospects and ability to raise additional financing to fund our operations.
We may not be able to reproduce the results of previously conducted clinical studies of other forms of KLK1, including Kailikang and Kallidinogenase, thereby preventing DM199 from displacing other forms of KLK1.
While there have been numerous studies demonstrating the efficacy of Kailikang and Kallidinogenase, we rely on the scientific and clinical knowledge and experience of other biotechnology and pharmaceutical companies and organizations in conducting those clinical studies. No assurance can be given that in our clinical trials involving DM199 we will be able to reproduce results of previously conducted studies or prove that DM199 is safe or effective and able to displace other forms of KLK1 in the market.
Negative results from clinical trials or studies of others and adverse safety events involving the targets of our product candidates may have an adverse impact on our future commercialization efforts.
From time to time, studies or clinical trials on various aspects of biopharmaceutical products are conducted by academic researchers, competitors, or others. The results of these studies or trials, when published, may have a significant effect on the market for the biopharmaceutical product that is the subject of the study. The publication of negative results of studies or clinical trials or adverse safety events related to our product candidates, or the therapeutic areas in which our product candidates compete, could adversely affect the market price of our common shares and our ability to finance future development of our product candidates, and our business and financial results could be materially and adversely affected.
We may be required to suspend, repeat or terminate our clinical trials if they are not conducted in accordance with regulatory requirements, the results are negative or inconclusive, or the trials are not well designed.
Clinical trials must be conducted in accordance with the FDA’s current Good Clinical Practices requirements, or cGCPs, or analogous requirements of applicable foreign regulatory authorities. Clinical trials are subject to oversight by the FDA, other foreign governmental agencies, and IRBs or ethics committees at the study sites where the clinical trials are conducted. In addition, clinical trials must be conducted with product candidates produced in accordance with applicable current Good Manufacturing Practices. Clinical trials may be suspended by us or by the FDA, other foreign regulatory authorities, or by an IRB or ethics committee with respect to a particular clinical trial site, for various reasons, including:
|
● |
deficiencies in the conduct of the clinical trials, including failure to conduct the clinical trial in accordance with regulatory requirements or study protocols; |
|
● |
deficiencies in the clinical trial operations or trial sites; |
|
● |
unforeseen adverse side effects or the emergence of undue risks to study subjects; |
|
● |
deficiencies in the trial design necessary to demonstrate efficacy; |
|
● |
the product candidate may not appear to offer benefits over current therapies; or |
|
● |
the quality or stability of the product candidate may fall below acceptable standards. |
The design and implementation of clinical trials is a complex process. As a Company, we have limited experience designing and implementing clinical trials. We may not successfully or cost-effectively design and implement clinical trials that achieve our desired clinical endpoints efficiently, or at all. A clinical trial that is not well designed may delay or even prevent initiation of the trial, can lead to increased difficulty in enrolling patients, may make it more difficult to obtain regulatory approval for the product candidate on the basis of the study results, or, even if a product candidate is approved, could make it more difficult to commercialize the product successfully or obtain reimbursement from third party payers. Additionally, a trial that is not well-designed could be inefficient or more expensive than it otherwise would have been, or we may incorrectly estimate the costs to implement the clinical trial, which could lead to a shortfall in funding.
Regulatory approval processes are lengthy, expensive, and inherently unpredictable. Our inability to obtain regulatory approval for our product candidates would substantially harm our business.
Our shareholders and investors should be aware of the risks, problems, delays, expenses, and difficulties which we may encounter in light of the extensive regulatory environment within which our business is carried out. Numerous statutes and regulations govern the preclinical and clinical development, manufacture and sale, and post-marketing responsibilities for non-therapeutic and human therapeutic products in the United States, European Union and other countries that are the intended markets for our current and future product candidates. Such legislation and regulations govern the approval of manufacturing facilities, the testing procedures, and controlled research that must be carried out, and the preclinical and clinical data that must be collected prior to marketing approval. Our R&D efforts, as well as any future clinical trials, and the manufacturing and marketing of any products we may develop, will be subject to and restricted by such extensive regulations.
The process of obtaining necessary regulatory approvals is lengthy, expensive, and uncertain. We may fail to obtain the necessary approvals to commence or continue clinical testing or to manufacture or market our potential products in reasonable time frames, if at all. In addition, governmental authorities in the United States or other countries may enact regulatory reforms or restrictions on the development of new therapies that could adversely affect the regulatory environment in which we operate or the development of any products we may develop.
Completing clinical testing and obtaining required approvals is expected to take several years and to require the expenditure of substantial resources. There can be no assurance that clinical trials will be completed successfully within any specified period of time, if at all. Furthermore, clinical trials may be delayed or suspended at any time by us or by the various regulatory authorities if it is determined at any time that the subjects or patients are being exposed to unacceptable risks.
Any failure or delay in obtaining regulatory approvals would adversely affect our ability to utilize our technology and would adversely affect our operations. Furthermore, no assurance can be given that our current or future product candidates will prove to be safe and effective in clinical trials or that they will receive the requisite regulatory approval. Moreover, any regulatory approval of a drug that is eventually obtained may be granted with specific limitations on the indicated uses for which that drug may be marketed. Furthermore, product approvals may be withdrawn if problems occur following initial marketing or if compliance with regulatory standards is not maintained.
Any product candidate for which we obtain marketing approval could be subject to post-marketing restrictions or recall or withdrawal from the market, and we may be subject to penalties if we fail to comply with regulatory requirements or if we experience unanticipated problems with our product candidates, when and if any of them are approved.
The FDA and other federal and state agencies, including the U.S. Department of Justice (DOJ), closely regulate compliance with all requirements governing prescription drug products, including requirements pertaining to marketing and promotion of drugs in accordance with the provisions of the approved labeling and manufacturing of products in accordance with cGMP requirements. The FDA and DOJ impose stringent restrictions on manufacturers’ communications regarding off-label use, and if we do not market our products for their approved indications, we may be subject to enforcement action for off-label marketing. Violations of such requirements may lead to investigations alleging violations of the Food, Drug and Cosmetic Act and other statutes, including the False Claims Act and other federal and state health care fraud and abuse laws as well as state consumer protection laws.
Our failure to comply with all regulatory requirements, and later discovery of previously unknown adverse events or other problems with our products, manufacturers or manufacturing processes, may yield various results, including:
|
● |
litigation involving patients using our products; |
|
● |
restrictions on such products, manufacturers or manufacturing processes; |
|
● |
restrictions on the labeling or marketing of a product; |
|
● |
restrictions on product distribution or use; |
|
● |
requirements to conduct post-marketing studies or clinical trials; |
|
● |
warning or untitled letters; |
|
● |
withdrawal of the products from the market; |
|
● |
refusal to approve pending applications or supplements to approved applications that we submit; |
|
● |
recall of products; |
|
● |
fines, restitution or disgorgement of profits or revenues; |
|
● |
suspension or withdrawal of marketing approvals; |
|
● |
damage to relationships with any potential collaborators; |
|
● |
unfavorable press coverage and damage to our reputation; |
|
● |
refusal to permit the import or export of our products; |
|
● |
product seizure; or |
|
● |
injunctions or the imposition of civil or criminal penalties. |
Non-compliance by us or any future collaborator with regulatory requirements regarding safety monitoring or pharmacovigilance, and with requirements related to the development of products for the pediatric population, can also result in significant financial penalties. Similarly, failure to comply with regulatory requirements regarding the protection of personal information can also lead to significant penalties and sanctions.
We may not achieve our publicly announced milestones according to schedule, or at all.
From time to time, we may announce the timing of certain events we expect to occur, such as the anticipated timing of initiation or completion of or results from our clinical trials. These statements are forward-looking and are based on the best estimates of management at the time relating to the occurrence of such events. However, the actual timing of such events may differ significantly from what has been publicly disclosed. The timing of events such as the initiation or completion of a clinical trial, filing of an application to obtain regulatory approval, or an announcement of additional clinical trials for a product candidate may ultimately vary from what is publicly disclosed. These variations in timing may occur as a result of different events, including the nature of the results obtained during a clinical trial or during a research phase, problems with a CMO or CRO or any other event having the effect of delaying the publicly announced timeline. We undertake no obligation to update or revise any forward-looking information, whether as a result of new information, future events or otherwise, except as otherwise required by law. Any variation in the timing of previously announced milestones could have a material adverse effect on our business plan, financial condition or operating results, and the trading price of our common shares.
Future development collaborations may be important to us. If we are unable to enter into or maintain these collaborations, or if these collaborations are not successful, our business could be adversely affected.
We may in the future determine to seek to collaborate with pharmaceutical and biotechnology companies for the development or commercialization of our current or future product candidates. We face significant competition in seeking appropriate collaborators. Our ability to reach a definitive agreement for any collaboration will depend, among other things, upon our assessment of the collaborator’s resources and expertise, the terms and conditions of the proposed collaboration and the proposed collaborator’s evaluation of a number of factors. If we are unable to reach agreements with suitable collaborators on a timely basis, on acceptable terms, or at all, we may have to curtail the development of a product candidate, reduce or delay its development program or one or more of our other development programs, delay its potential development schedule or reduce the scope of research activities, or increase our expenditures and undertake discovery, nonclinical or clinical development activities at our own expense. If we fail to enter into collaborations and do not have sufficient funds or expertise to undertake the necessary development activities, we may not be able to continue or further develop our current or future product candidates, and our business may be materially and adversely affected.
Future collaborations we may enter into may involve the following risks, among others:
|
● |
collaborators may have significant discretion in determining the efforts and resources that they will apply to these collaborations; |
|
● |
collaborators may not perform their obligations as expected; |
|
● |
changes in the collaborators’ strategic focus or available funding, or external factors, such as an acquisition, may divert resources or create competing priorities; |
|
● |
collaborators may delay discovery, nonclinical or clinical development, provide insufficient funding for product development of targets selected by us, stop or abandon discovery, nonclinical or clinical development for a product candidate, or repeat or conduct new discovery, and nonclinical and clinical development for a product candidate; |
|
● |
collaborators could independently develop, or develop with third parties, products that compete directly or indirectly with our products or product candidates if the collaborators believe that competitive products are more likely to be successfully developed than our products; |
|
● |
product candidates discovered in collaboration with us may be viewed by our future collaborators as competitive with their own product candidates or products, which may cause collaborators to cease to devote resources to the development of our product candidates; |
|
● |
disagreements with collaborators, including disagreements over proprietary rights, contract interpretation or the preferred course of development, might cause delays or termination of the discovery, preclinical or clinical development or commercialization of product candidates, might lead to additional responsibilities for us with respect to product candidates, or might result in litigation or arbitration, any of which would be time-consuming and expensive; |
|
● |
collaborators may not properly maintain or defend our intellectual property rights or intellectual property rights licensed to us or may use our proprietary information in such a way as to invite litigation that could jeopardize or invalidate our intellectual property or proprietary information or expose us to potential litigation; |
|
● |
collaborators may infringe the intellectual property rights of third parties, which may expose us to litigation and potential liability; and |
|
● |
collaborations may be terminated for the convenience of the collaborator and, if terminated, we could be required to raise additional capital to pursue further development or commercialization of the applicable product candidates. |
Additionally, subject to its contractual obligations to us, if a collaborator is involved in a business combination, the collaborator might deemphasize or terminate the development of any of our product candidates. If a collaborator terminates its agreement with us, we may find it more difficult to attract new collaborators and the way we are perceived in the business and financial communities could be adversely affected.
If our collaborations do not result in the successful development of our product candidates, our product candidates could be delayed and we may need additional resources to develop product candidates. All of the risks relating to product development, regulatory approval and commercialization described in this report also apply to the activities of our future collaborators.
The successful commercialization of our current or future product candidates, if approved, will depend on achieving market acceptance and we may not be able to gain sufficient acceptance to generate significant revenue.
Even if our product candidates are successfully developed and receive regulatory approval, they may not gain market acceptance among physicians, patients, healthcare payers such as private insurers or governments and other funding parties, and the medical community. The degree of market acceptance for any products we develop will depend on a number of factors including, among others:
|
● |
demonstration of the clinical efficacy and safety; |
|
● |
the prevalence and severity of any adverse side effects; |
|
● |
limitations or warnings contained in the product’s approved labeling; |
|
● |
cost-effectiveness and availability of acceptable pricing; |
|
● |
competitive product profile versus alternative treatment methods and the superiority of alternative treatment or therapeutics; |
|
● |
the effectiveness of marketing and distribution methods and support for the products; and |
|
● |
coverage and reimbursement policies of government and third-party payers to the extent that our products could receive regulatory approval but not be approved for coverage by or receive adequate reimbursement from government and quasi-government agencies or other third-party payers. |
Disease indications may be small subsets of a disease that could be parsed into smaller and smaller indications as different subsets of diseases are defined. This increasingly fine characterization of diseases could have negative consequences, including creating an approved indication that is so small as not to have a viable market for us. If future technology allows characterization of a disease in a way that is different from the characterization used for large, pivotal studies, it may make those studies invalid or reduce their usefulness, and may require repeating all or a portion of the studies. Future technology may supply better prognostic ability, which could reduce the portion of patients projected to need a new therapy. Even after being cleared by regulatory authorities, a product may later be shown to be unsafe or not to have its purported effect, thereby preventing its widespread use or requiring withdrawal from the market.
If we fail to obtain coverage and adequate reimbursement for our products, our revenue-generating ability will be diminished and there is no assurance that the anticipated market for our products will be sustained.
We believe that there may be many different potential applications for products successfully derived from our technologies and that the anticipated market for products under development will continue to expand. However, due to competition from existing or new products and the yet-to-be established commercial viability of our product candidates, no assurance can be given that these beliefs will prove to be correct. Physicians, patients, formularies, payers or the medical community in general may not accept or utilize any products that we may develop. Other drugs may be approved during our clinical testing which could change the accepted treatments for the diseases we have targeted and make our product candidates obsolete.
Our ability to successfully commercialize our future products, if any, will depend, in part, on the extent to which coverage of and adequate reimbursement for such products and related treatments will be available from governmental health payer programs at the federal and state levels, including Medicare and Medicaid, private health insurers, managed care plans and other organizations. No assurance can be given that third-party coverage and adequate reimbursement will be available that will allow us to obtain or maintain price levels sufficient for the realization of an appropriate return on our investment in product development. Coverage and adequate reimbursement from governmental healthcare programs, such as Medicare and Medicaid, and private health insurers, managed care plans and other organizations is critical to new product acceptance by healthcare providers. There is no uniform coverage and reimbursement policy among third-party payers in the United States; however, private third-party payers may follow Medicare coverage and reimbursement policy in setting their own coverage policy and reimbursement rates. Additionally, coverage decisions may depend upon clinical and economic standards that disfavor new drug products when more established or lower cost therapeutic alternatives are already available or subsequently become available. Even if we obtain coverage for our product candidates, the related reimbursement rates might not be adequate to make our product attractive to providers, or may require patient cost sharing (e.g., copayments/deductibles) that patients find unacceptably high. In addition, healthcare reform and controls on healthcare spending may limit coverage of our products and the price we charge and get paid for any products and the amounts thereof that we can sell. Patients are unlikely to use our product candidates unless coverage is provided and reimbursement is adequate to cover a significant portion of the cost of our product candidates.
Outside of the United States, the successful commercialization of our products will depend largely on obtaining and maintaining government coverage, because in many countries patients are unlikely to use prescription drugs that are not covered by their government healthcare programs. Negotiating coverage and reimbursement with governmental authorities can delay commercialization by 12 months or more. Coverage and reimbursement policies may adversely affect our ability to sell our products on a profitable basis. In many international markets, governments control the prices of prescription pharmaceuticals, including through the implementation of reference pricing, price cuts, rebates, revenue-related taxes and profit control, and we expect prices of prescription pharmaceuticals to decline over the life of the product or as volumes increase.
We will not be able to successfully commercialize our current or future product candidates without establishing sales and marketing capabilities internally or through collaborators.
We currently have no sales and marketing staff. We may not be able to find suitable sales and marketing staff and collaborators for our products if and when they receive required approvals. We have no prior experience in the marketing, sale and distribution of pharmaceutical products, and there are significant risks involved in building and managing a sales organization, including our ability to hire, retain and incentivize qualified individuals, generate sufficient sales leads, provide adequate training to sales and marketing personnel, effectively manage a geographically dispersed sales and marketing team, and maintain compliance by a marketing team with complex laws and regulations applicable to product marketing. Any collaborators may not be adequate or successful or could terminate or materially reduce the effort they direct to our products. The development of a marketing and sales capability will require significant expenditures, management resources and time. The cost of establishing such a sales force may exceed any potential product revenue, or our marketing and sales efforts may be unsuccessful. If we are unable to develop an internal marketing and sales capability in a timely fashion, or at all, or if we are unable to enter into a marketing and sales arrangement with a third party on acceptable terms, we may be unable to successfully develop and seek regulatory approval for our product candidates and/or effectively market and sell approved products, if any.
We face competition from other biotechnology and pharmaceutical companies and our financial condition and operations will suffer if we fail to compete effectively.
Technological competition is intense in the industry in which we operate. Competition comes from pharmaceutical companies, biotechnology companies, and universities, as well as companies that offer non-pharmaceutical solutions in the markets we may attempt to address with our products. Many of our competitors have substantially greater financial and technical resources; more extensive R&D capabilities; and greater marketing, distribution, production, and human resources than we do. Moreover, competitors may develop products more quickly than us and may obtain regulatory approval for such products more rapidly than we do. Products and processes which are more effective than those that we intend to develop may be developed by our competitors. R&D by others may render our product candidates non-competitive or obsolete.
Our product candidates may face competition sooner than expected.
We believe that DM199 could qualify for 12 years of data exclusivity in the United States under the Biologics Price Competition and Innovation Act of 2009, which was enacted as part of the ACA. Under the BPCIA, an application for a biosimilar product, or BLA, cannot be submitted to the FDA until four years, or if approved by the FDA, until 12 years, after the original brand product identified as the reference product is approved under a BLA. The BPCIA provides an abbreviated pathway for the approval of biosimilar and interchangeable biological products. The new abbreviated regulatory pathway establishes legal authority for the FDA to review and approve biosimilar biologics, including the possible designation of a biosimilar as “interchangeable” based on its similarity to an existing brand product. This law is complex and is only beginning to be interpreted and implemented by the FDA. While it is uncertain when any such processes may be fully adopted by the FDA, any such processes could have a material adverse effect on the future commercial prospects for any of our product candidates that are biologics. There is also a risk that the U.S. Congress could repeal or amend the BPCIA to shorten this exclusivity period, potentially creating the opportunity for biosimilar competition sooner than anticipated after the expiration of our patent protection. Moreover, the extent to which a biosimilar, once approved, will be substituted for any reference product in a way that is similar to traditional generic substitution for non-biological products is not yet clear, and will depend on a number of marketplace and regulatory factors that are still developing.
Even if, as we expect, our current or future product candidates are considered to be reference products eligible for 12 years of exclusivity under the BPCIA, another company could market competing products if the FDA approves a full BLA for such product containing the sponsor’s own preclinical data and data from adequate and well-controlled clinical trials to demonstrate the safety, purity and potency of the products. Moreover, an amendment or repeal of the BPCIA could result in a shorter exclusivity period for our product candidates, which could have a material adverse effect on our business.
Our relationships with customers and third-party payers will be subject to applicable fraud and abuse and other healthcare laws and regulations, which could expose us to criminal sanctions, civil penalties, program exclusion, contractual damages, reputational harm and diminished profits and future earnings.
Healthcare providers, physicians and third-party payers will likely play a primary role in the recommendation, prescription and sale of any product candidates for which we receive marketing approval. Our future arrangements with third-party payers, customers and prescribing providers may expose us to broadly applicable fraud and abuse and other healthcare laws and regulations that may constrain the business or financial arrangements and relationships through which we market, distribute and sell the products for which we receive marketing approval. Currently, applicable federal and state healthcare laws and regulations that may apply to our products and arrangements include the following:
|
● |
the federal healthcare anti-kickback statute prohibits, among other things, persons from knowingly and willfully soliciting, offering, receiving or providing remuneration, directly or indirectly, in cash or in kind, to induce or reward either the referral of an individual for, or the purchase, order or recommendation of, any good or service, for which payment may be made under federal and state healthcare programs such as Medicare and Medicaid. This statute may apply to our marketing practices, educational programs, pricing policies and relationships with healthcare providers in a position to prescribe or recommend our products. A person or entity does not need to have actual knowledge of this statute or specific intent to violate it in order to have committed a violation; |
|
● |
the federal False Claims Act imposes civil penalties, including civil whistleblower or qui tam actions, against individuals or entities for knowingly presenting, or causing to be presented, to the federal government, claims for payment that are false or fraudulent or making a false statement to avoid, decrease or conceal an obligation to pay money to the federal government. The government also may assert that a claim including items or services resulting from a violation of the federal Anti-Kickback Statute constitutes a false or fraudulent claim for purposes of the false claims statutes. Pharmaceutical and other healthcare companies have been prosecuted under these laws for, among other things, allegedly inflating drug prices they report to pricing services, which in turn were used by the government to set Medicare and Medicaid reimbursement rates, and for allegedly providing free product to customers with the expectation that the customers would bill federal programs for the product. In addition, certain marketing practices, including off-label promotion, may also violate false claims laws; |
|
● |
the federal Health Insurance Portability and Accountability Act of 1996 (HIPAA), as amended by the Health Information Technology for Economic and Clinical Health Act, imposes criminal and civil liability for executing a scheme to defraud any healthcare benefit program and also imposes obligations, including mandatory contractual terms, with respect to safeguarding the privacy, security and transmission of individually identifiable health information. There is an increasing trend for more criminal prosecutions and compliance enforcement activities for noncompliance with HIPAA as well as for data breaches involving protected individually identifiable health information. In the ordinary course of our business, we may receive protected health information from clinical study sites and clinicians. HIPAA restricts the use and disclosure of health information by most health care providers (Covered Entities) as well as by individuals and entities that perform various functions for or on behalf of Covered Entities (Business Associates). Depending on how we engage with health care providers in the development and commercialization of products, we may be deemed to be a Business Associate under HIPAA. Failure to comply with the HIPAA privacy and security standards may subject us to civil and criminal liability, and the cost of reporting and mitigating data breaches could be significant, all of which could have a material adverse effect on us and our operating results; |
|
● |
the federal false statements statute prohibits knowingly and willfully falsifying, concealing or covering up a material fact or making any materially false statement in connection with the delivery of or payment for healthcare benefits, items or services; |
|
● |
the federal Physician Payments Sunshine Act under the ACA requires manufacturers of drugs, devices, biologics and medical supplies for which payment is available under Medicare, Medicaid or the Children’s Health Insurance Program (with certain exceptions) to report annually to the Centers for Medicare & Medicaid Services (CMS) information related to payments or other “transfers of value” made to physicians (defined to include doctors, dentists, optometrists, podiatrists and chiropractors) and teaching hospitals, and requires applicable manufacturers and group purchasing organizations to report annually to CMS ownership and investment interests held by the physicians and their immediate family members and payments or other “transfers of value” to such physician owners. Effective January 2022, applicable manufacturers will also be required to collect and report information on payments or “transfers of value” to physician assistants, nurse practitioners, clinical nurse specialists, certified registered nurse anesthetists, and certified nurse-midwives; |
|
● |
analogous state laws and regulations, such as state anti-kickback and false claims laws, may apply to sales or marketing arrangements and claims involving healthcare items or services reimbursed by non-governmental third-party payers, including private insurers, and some state laws require pharmaceutical companies to comply with the pharmaceutical industry’s voluntary compliance guidelines and the relevant compliance guidance promulgated by the federal government in addition to requiring drug manufacturers to report information related to payments to physicians and other healthcare providers or marketing expenditures; |
|
● |
the distribution of prescription pharmaceutical products is subject to the Prescription Drug Marketing Act (PDMA) and its implementation regulations, as well as the Drug Supply Chain Security Act (DSCSA), which regulates the distribution of and tracing of prescription drugs and prescription drug samples at the federal level, and sets minimum standards for the regulation of drug distributors by the states. The PDMA, its implementing regulations and state laws limit the distribution of prescription pharmaceutical product samples, and the DSCSA imposes requirements to ensure accountability in distribution and to identify and remove counterfeit and other illegitimate products from the market; and |
|
● |
the U.S. Foreign Corrupt Practices Act of 1977, as amended (FCPA), the U.S. domestic bribery statute contained in 18 U.S.C. §201 and the U.S. Travel Act. |
Some state laws require pharmaceutical companies to comply with the pharmaceutical industry’s voluntary compliance guidelines and the relevant compliance guidance promulgated by the federal government and may require drug manufacturers to report information related to payments and other transfers of value to physicians and other healthcare providers or marketing expenditures. State and foreign laws also govern the privacy and security of health information in some circumstances, many of which differ from each other in significant ways and often are not preempted by HIPAA, thus complicating compliance efforts.
The risk of our being found in violation of these laws and regulations is increased by the fact that many of them have not been fully interpreted by the regulatory authorities or the courts, and their provisions are open to a variety of interpretations. We are unable to predict what additional federal or state legislation or regulatory initiatives may be enacted in the future regarding our business or the healthcare industry in general, or what effect such legislation or regulations may have on us. Federal or state governments may impose additional restrictions or adopt interpretations of existing laws that could have a material adverse effect on us. Although we will endeavor to identify and comply with new laws and regulations and new interpretations of existing laws and regulations, it is possible that we may be unaware of new legal requirements or interpretations, which could result in our violation of these laws and/or regulations.
Laws, restrictions, and other regulatory measures are also imposed by anti-kickback prohibitions, fraud and abuse restrictions, and other healthcare laws and regulations in international jurisdictions, and in those jurisdictions, we face the same issues as in the United State regarding exposure to criminal sanctions, civil penalties, program exclusion, contractual damages, reputational harm, and diminished profits and future earnings.
Efforts to ensure that our business arrangements with third parties will comply with applicable healthcare laws and regulations will involve substantial costs. It is possible that governmental authorities will conclude that our business practices may not comply with current or future statutes, regulations or case law involving applicable fraud and abuse or other healthcare laws and regulations. Some of these laws may have safe harbors and/or exceptions that, if met, may protect our arrangements from liability. However, failure to meet any element of a safe harbor or exception may cause an arrangement to lose safe harbor/exception protection. There may not be safe harbors or exceptions for every potential financial arrangement we may enter into, and there can be no assurances that any of our arrangements or relationships will meet an otherwise applicable safe harbor or exception.
If our operations are found to be in violation of any of these laws or any other governmental regulations that may apply to us, we may be subject to significant civil, criminal and administrative penalties, damages, fines, exclusion from government funded healthcare programs, such as Medicare and Medicaid, and the curtailment or restructuring of our operations. If any of the physicians or other providers or entities with whom we expect to do business are found to be not in compliance with applicable laws, they may be subject to criminal, civil or administrative sanctions, including exclusions from government funded healthcare programs. Any investigation of or action against us for violation of these laws, even if we successfully defend against it, would cause us to incur significant legal expenses and divert our management’s attention from the operation of our business.
We heavily rely on the capabilities and experience of our key executives and scientists and the loss of any of them could affect our ability to develop our products.
We depend heavily on members of our management team and certain other key personnel, including in particular our clinical personnel. We also depend on our clinical collaborators and advisors, all of whom have outside commitments that may limit their availability to us. In addition, we believe that our future success will depend in large part upon our ability to attract and retain highly skilled scientific, managerial, medical, clinical, and regulatory personnel, particularly as we continue to expand our activities and seek regulatory approvals for clinical trials and eventually our DM199 product candidate. We enter into agreements with scientific and clinical collaborators and advisors, key opinion leaders, and academic partners in the ordinary course of our business. We also enter into agreements with physicians and institutions that will recruit patients into our clinical trials on our behalf in the ordinary course of our business. Notwithstanding these arrangements, we face significant competition for these types of personnel from other companies, research and academic institutions, government entities and other organizations. We cannot predict our success in hiring or retaining the personnel we require for continued growth. The loss of the services of any of our executive officers or other key personnel could potentially harm our business, operating results, or financial condition.
We will likely need to expand our operations and increase the size of our company, and we may experience difficulties in managing growth.
As we advance DM199 and any future product candidates through preclinical testing and clinical studies, and develop our current or future product candidates, we will need to increase our product development, scientific, regulatory and compliance and administrative headcount to manage these programs. In addition, to continue to meet our obligations as a public company, we will likely need to increase our general and administrative capabilities. Our management, personnel and systems currently in place may not be adequate to support this future growth. Our need to effectively manage our operations, growth and various projects requires that we:
|
● |
successfully attract and recruit new employees with the expertise and experience we will require; |
|
● |
manage our clinical programs effectively, which we anticipate being conducted at numerous clinical sites; |
|
● |
develop a marketing, distribution and sales infrastructure if we seek to market our products directly; and |
|
● |
continue to improve our operational, manufacturing, quality assurance, financial and management controls, reporting systems and procedures. |
If we are unable to successfully manage this growth and increased complexity of operations, our business may be adversely affected.
Our employees may engage in misconduct or other improper activities, including noncompliance with regulatory standards and requirements, which could have a material adverse effect on our business.
We are exposed to the risk of employee fraud or other misconduct. Misconduct by employees could include failure to comply with FDA regulations, provide accurate information to the FDA, comply with manufacturing and reporting standards we have established, comply with federal and state health-care fraud and abuse laws and regulations, report financial information or data accurately, or disclose unauthorized activities to us. In particular, sales, marketing, and business arrangements in the healthcare industry are subject to extensive laws and regulations intended to prevent fraud, kickbacks, self-dealing, and other abusive practices. These laws and regulations may restrict or prohibit a wide range of pricing, discounting, marketing and promotion, sales commission, customer incentive programs, and other business arrangements. Employee misconduct could also involve the improper use of information obtained in the course of clinical trials, which could result in regulatory sanctions and serious harm to our reputation. If any such actions are instituted against us, and we are not successful in defending ourselves or asserting our rights, those actions could have a substantial impact on our business and results of operations, including the imposition of substantial fines or other sanctions. Even if we are successful in defending against any such action, we would incur significant legal expenses in responding to and defending against it.
We may expand our business through the acquisition of companies or businesses or by entering into collaborations or by in-licensing product candidates, each of which could disrupt our business and harm our financial condition.
We have in the past and may in the future seek to expand our pipeline and capabilities by acquiring one or more companies or businesses, entering into collaborations, or in-licensing one or more technologies or product candidates. Our ability to grow through acquisitions, collaborations and in-licenses will depend, in part, on the availability of suitable candidates at acceptable prices, terms and conditions, our ability to compete effectively for candidates, and the availability of capital and personnel resources to carry out such transactions. Acquisitions, collaborations and in-licenses involve numerous risks, including, among others:
|
● |
substantial cash expenditures; |
|
● |
adverse impact on overall profitability; |
|
● |
technology development risks; |
|
● |
potentially dilutive issuances of equity securities; |
|
● |
reallocation of amounts of capital from other initiatives; |
|
● |
incurrence of debt and contingent liabilities, some of which may be difficult or impossible to identify at the time of acquisition; |
|
● |
write-off of significant amounts of goodwill, other intangible assets and/or long-lived assets as a result of deterioration in the performance of an acquired business, adverse market conditions, changes in the competitive landscape, changes in laws or regulations that restrict activities of an acquired business, or as a result of a variety of other circumstances; |
|
● |
difficulties in assimilating the information and financial systems, operations, processes and products of the acquired companies; |
|
● |
inability to effectively manage our expanded operations; |
|
● |
potential disputes regarding contingent consideration; |
|
● |
diverting our management’s attention away from other business concerns; |
|
● |
disruption to our existing operations and plans; |
|
● |
entering markets in which we have limited or no direct experience; |
|
● |
potential loss of our key employees or key employees of the acquired companies or businesses; |
|
● |
violation of confidentiality, intellectual property, and non-compete obligations or agreements by employees of an acquired business or lack of or inadequate formal intellectual property protection mechanisms in place at an acquired business; |
|
● |
failure by acquired businesses to comply with applicable international, federal and state regulatory standards; |
|
● |
infringement by acquired businesses of intellectual property rights of others; |
|
● |
inaccurate assessment of additional post-acquisition or business venture investments, undisclosed, contingent or other liabilities or problems, unanticipated costs associated with an acquisition, and an inability to recover or manage such liabilities and costs; and |
|
● |
incorrect estimates made in the accounting for acquisitions and incurrence of non-recurring charges. |
We cannot provide assurance that any acquisition, collaboration, or in-license will result in short-term or long-term benefits to us. We may incorrectly judge the value or worth of an acquired company or business or in-licensed product candidate. In addition, our future success would depend in part on our ability to manage the growth associated with some of these acquisitions, collaborations and in-licenses. We cannot provide assurance that we would be able to successfully combine our business with that of acquired businesses, manage a collaboration or integrate in-licensed product candidates. Furthermore, the development or expansion of our business may require a substantial capital investment by us.
Our DM199 product candidate or future product candidates may cause or have attributed to them undesirable side effects or have other properties that could delay or prevent their regulatory approval, limit the commercial scope of their approved uses, or result in significant negative consequences following any marketing approval.
Undesirable side effects caused by our DM199 product candidate or any future product candidate or that may be identified as related to our product candidates by investigators conducting our clinical trials or even related to competing products in development that use a similar mechanism of action or act through a similar biological disease pathway could cause us or regulatory authorities to interrupt, delay or halt clinical trials and could result in the delay or denial of regulatory approval by the FDA or other comparable foreign regulatory authorities, potential product liability claims or a more restrictive label. Results of our trials could reveal unacceptable side effects or unexpected characteristics which could be attributed to our DM199 product candidate or any future product candidates. This may require longer and more extensive clinical development or we could suspend or terminate our clinical trials or the FDA or comparable foreign regulatory authorities could order us to cease clinical trials or deny approval of our product candidates for any or all of our targeted indications. Drug-related side effects could affect patient recruitment or the ability of enrolled subjects to complete the trial or result in potential product liability claims. Any of these occurrences may harm our business, financial condition and prospects significantly.
Additionally, if one or more of our product candidates receives marketing approval, and we or others later identify undesirable side effects caused by any such products, a number of potentially significant negative consequences could result, including, among others:
|
● |
we may suspend marketing of, or withdraw or recall, such product; |
|
● |
regulatory authorities may withdraw approvals of such product; |
|
● |
regulatory authorities may require additional warnings on the label or otherwise seek to limit the scope of the approved uses reflected in the label of such product; |
|
● |
the FDA may require the use of or modification of a Risk Evaluation and Mitigation Strategy (REMS) or a comparable foreign regulatory authority may require the establishment or modification of a similar strategy that may, for instance, restrict distribution of our products and impose other implementation requirements on us; |
|
● |
regulatory authorities may require that we conduct post-marketing studies; |
|
● |
we could be sued and held liable for harm caused to patients; and |
|
● |
our reputation may suffer. |
Any of these events could prevent us from achieving or maintaining market acceptance of the particular product candidate or otherwise materially harm the commercial prospects for the product candidate, if approved, and could significantly harm our business, results of operations and prospects.
We face the risk of product liability claims, which could exceed our insurance coverage and produce recalls, each of which could deplete our cash resources.
We are exposed to the risk of product liability claims alleging that use of our product candidates caused an injury or harm. These claims can arise at any point in the development, testing, manufacture, marketing, or sale of our product candidates and may be made directly by patients involved in clinical trials of our product candidates, by consumers or healthcare providers, or by individuals, organizations, or companies selling our products. Product liability claims can be expensive to defend, even if the product or product candidate did not actually cause the alleged injury or harm.
Insurance covering product liability claims becomes increasingly expensive as a product candidate moves through the development pipeline to commercialization. To protect against potential product liability risks, we have AUD $20 million per occurrence and AUD $20 million aggregate clinical trial insurance for the REMEDY Phase II clinical trial in Australia and US $5.0 million product liability insurance coverage. However, there can be no assurance that such insurance coverage is or will continue to be adequate or available to us at a cost acceptable to us or at all. We may choose or find it necessary under our collaboration agreements to increase our insurance coverage in the future. We may not be able to secure greater or broader product liability insurance coverage on acceptable terms or at reasonable costs when needed. Any liability for damages resulting from a product liability claim could exceed the amount of our coverage, require us to pay a substantial monetary award from our own cash resources and have a material adverse effect on our business, financial condition, and results of operations. Moreover, a product recall, if required, could generate substantial negative publicity about our products and business, inhibit or prevent commercialization of other products and product candidates, or negatively impact existing or future collaborations.
If we are unable to maintain product liability insurance required by our third parties, the corresponding agreements would be subject to termination, which could have a material adverse impact on our operations.
Some of our license, clinical trials and other agreements with third parties require, and in the future will likely require, us to maintain product liability insurance in at least certain specified minimum amounts. If we cannot maintain acceptable amounts of coverage on commercially reasonable terms in accordance with the terms set forth in these agreements, the corresponding agreements would be subject to termination, which could have a material adverse impact on our operations.
A risk of product liability claims, and related negative publicity, is inherent in the development of human therapeutics and other products. Product liability insurance is expensive, its availability is limited, and it may not be offered on terms acceptable to us, or at all. The commercialization of our potential products could be inhibited or prevented by an inability to maintain sufficient insurance coverage on reasonable terms or to otherwise protect against potential product liability claims. A product liability claim against us or the withdrawal of a product from the market could have a material adverse effect upon us and our financial condition.
A variety of risks are associated with operating our business internationally which could materially adversely affect our business.
We currently conduct certain R&D operations in the United States and Australia. In the future, we expect to conduct certain clinical trials, and plan to seek regulatory approval of our product candidates, outside of the United States. Accordingly, we are subject to risks related to operating in foreign countries including, among others:
|
● |
different regulatory requirements for drug approvals in foreign countries; |
|
● |
different standards of care in various countries that could complicate the evaluation of our product candidates; |
|
● |
different United States and foreign drug import and export rules; |
|
● |
reduced protection for intellectual property rights in certain countries; |
|
● |
withdrawal from or revision to international trade policies or agreements and the imposition or increases in import and export licensing and other compliance requirements, customs duties and tariffs, import and export quotas and other trade restrictions, license obligations, and other non-tariff barriers to trade; |
|
● |
unexpected changes in tariffs, trade barriers, and regulatory requirements; |
|
● |
the imposition of U.S. or international sanctions against a country, company, person, or entity with whom we do business that would restrict or prohibit continued business with that country, company, person, or entity; |
|
● |
different reimbursement systems and different competitive drugs indicated to treat the indications for which our product candidates are being developed; |
|
● |
economic weakness, including inflation, or political instability in particular foreign economies and markets; |
|
● |
compliance with tax, employment, immigration, and labor laws for employees living or traveling abroad; |
|
● |
compliance with the Foreign Corrupt Practices Act and other anti-corruption and anti-bribery laws; |
|
● |
foreign taxes, including withholding of payroll taxes; |
|
● |
foreign currency exchange rate fluctuations, which could result in increased operating expenses and/or reduced revenue, and other obligations incident to doing business in another country; |
|
● |
difficulties in managing and staffing international operations and increases in infrastructure costs, including legal, tax, accounting, and information technology; |
|
● |
workforce uncertainty in countries where labor unrest is more common than in the United States; |
|
● |
production shortages resulting from any events affecting raw material supply or manufacturing capabilities abroad; |
|
● |
potential liability resulting from development work conducted by foreign partners; |
|
● |
transportation delays and interruptions; |
|
● |
business interruptions resulting from natural disasters or geopolitical actions, including war and terrorism, or systems failure, including cybersecurity breaches; and |
|
● |
compliance with evolving and expansive international data privacy laws, such as the European Union General Data Protection Regulation. |
Future legislation in the United States, Europe or other countries, and/or regulations and policies adopted by the FDA, the EMA or comparable regulatory authorities, may increase the time and cost required for us or our collaborator to conduct and complete clinical trials of our current or future product candidates.
The FDA and the EMA have each established regulations to govern the product development and approval process, as have other foreign regulatory authorities. The policies of the FDA, the EMA and other regulatory authorities may change. For example, in December 2016, the 21st Century Cures Act (Cures Act) was signed into law. The Cures Act, among other things, is intended to modernize the regulation of drugs and spur innovation, but not all of its provisions have yet been implemented. Additionally, in August 2017, the FDA issued final guidance setting forth its current thinking with respect to development programs and clinical trial designs for antibacterial drugs to treat serious bacterial diseases in patients with an unmet medical need. We cannot predict what if any effect the Cures Act or any existing or future guidance from the FDA or other regulatory authorities will have on the development of our product candidates.
Recently enacted and future legislation may increase the difficulty and cost for us and our future collaborators to obtain marketing approval of and commercialize our product candidates and affect the prices we may obtain.
In the United States and some foreign jurisdictions, there have been a number of legislative and regulatory changes and proposed changes regarding the healthcare system that could prevent or delay marketing approval of our product candidates, restrict or regulate post-approval activities and affect our ability to profitably sell any product candidates for which we obtain marketing approval.
Among policy makers and payers in the United States and elsewhere, there is significant interest in promoting changes in healthcare systems with the stated goals of containing healthcare costs, improving quality and/or expanding access. For example, the ACA, which was enacted in the United States in March 2010, includes measures to change health care delivery, decrease the number of individuals without insurance, ensure access to certain basic health care services, and contain the rising cost of care. This healthcare reform movement, including the enactment of the ACA, has significantly changed health care financing by both governmental and private insurers in the United States. With respect to pharmaceutical manufacturers, the ACA increased the number of individuals with access to health care coverage, including prescription drug coverage, but it simultaneously imposed, among other things, increased liability for rebates and discounts owed to certain entities and government health care programs, fees for the manufacture or importation of certain branded drugs, and transparency reporting requirements under the Physician Payments Sunshine Act.
Since its enactment, there have been judicial and Congressional challenges to certain aspects of the ACA, as well as efforts by the current administration to repeal or replace certain aspects of the ACA. Since January 2017, two U.S. Presidential Executive Orders have been signed and other directives designed to delay the implementation of certain provisions of the ACA or otherwise remove some of the requirements for health insurance mandated by the ACA. Concurrently, Congress has considered legislation that would repeal or repeal and replace all or part of the ACA. While Congress has not passed comprehensive repeal legislation, two bills affecting the implementation of certain taxes under the ACA have been signed into law. The Tax Cuts and Jobs Act of 2017 includes a provision repealing, effective January 1, 2019, the tax-based individual shared responsibility payment imposed by the ACA on certain individuals who fail to maintain qualifying health coverage for all or part of a year, which is commonly referred to as the “individual mandate.” Additionally, on January 22, 2018, the U.S. President signed a continuing resolution on appropriations for fiscal year 2018. This continuing resolution delayed implementation of the tax on certain high cost employer-sponsored insurance plans until January 1, 2022 and provided a moratorium on the annual fee imposed on certain health insurance providers based on market share until January 1, 2020. Further, the Bipartisan Budget Act of 2018, among other things, amended the ACA, effective January 1, 2019, to increase from 50 percent to 70 percent the point-of-sale discount that is owed by pharmaceutical manufacturers who participate in Medicare Part D and to close the coverage gap in most Medicare drug plans, commonly referred to as the “donut hole.”
In addition to the ACA, other federal health reform measures have been proposed and adopted in the United States. For example, legislation has been enacted to reduce the level of reimbursement paid to providers under the Medicare program over time, as well as to phase in alternative payment models for provider services under the Medicare program with the goal of incentivizing the attainment of pre-defined quality measures. As these measures are not fully in effect, and since the U.S. Congress could intervene to prevent their full implementation, it is unclear how payment reductions or the introduction of the quality payment program will impact overall physician reimbursement under the Medicare program. It is also unclear if changes in Medicare payments to providers would impact such providers’ willingness to prescribe and administer our products, if approved. Further, there has been heightened governmental scrutiny over the manner in which companies set prices for their marketed products. For example, there have been several recent Congressional inquiries and proposed and enacted federal and state legislation designed to, among other things, bring more transparency to drug pricing, review the relationship between pricing and patient programs, and reform government program reimbursement methodologies for drug products.
We expect that the ACA, as well as other healthcare reform measures that may be adopted in the future, may result in more rigorous coverage criteria and additional downward pressure on the price that we may receive for any product, if approved. Any reduction in reimbursement from Medicare or other government programs may result in a similar reduction in payments from private payers. The implementation of cost containment measures or other healthcare reforms may prevent us from being able to generate revenue, attain profitability, or commercialize our product candidates.
Legislative and regulatory proposals have been made to expand post-approval requirements and restrict sales and promotional activities for drugs. We cannot be sure whether additional legislative changes will be enacted, or whether the FDA regulations, guidance or interpretations will be changed, or what the impact of such changes on the marketing approvals of our current or future product candidates, if any, may be. In addition, increased scrutiny by the U.S. Congress of the FDA’s approval process may significantly delay or prevent marketing approval, as well as subject us to more stringent product labeling and post-marketing testing and other requirements.
Our inability to maintain contractual relationships with physicians could have a negative impact on our research and development.
We maintain contractual relationships with respected physicians in hospitals and universities who assist us in the design of our clinical trials and interpretation of trial results. If we are unable to enter into and maintain these relationships, our ability to develop, obtain required regulatory approvals for, and market our product candidates could be adversely affected. In addition, it is possible that U.S. federal and state and international laws requiring us to disclose payments or other transfers of value, such as free gifts or meals, to surgeons and other healthcare providers could have a chilling effect on these relationships with individuals or entities that may, among other things, want to avoid public scrutiny of their financial relationships with us.
We conduct certain research and development operations through our Australian wholly-owned subsidiary. If we lose our ability to operate in Australia, or if our subsidiary is unable to receive the research and development incentive payment allowed by Australian regulations, our business and results of operations could suffer.
We maintain a wholly-owned Australian subsidiary, DiaMedica Australia Pty Ltd., to conduct various clinical activities for our product and development candidate in Australia. Due to the geographical distance and lack of employees currently in Australia, as well as our lack of experience operating in Australia, we may not be able to efficiently or successfully monitor, develop and commercialize our lead product candidate in Australia, including conducting clinical trials. Furthermore, we have no assurance that the results of any clinical trials that we conduct for our product candidate in Australia will be accepted by the FDA or foreign regulatory authorities for development and commercialization approvals.
In addition, current Australian tax regulations provide for a refundable R&D incentive payment equal to 43.5% of qualified expenditures. We received incentive payments of approximately USD $856,000 and USD $621,000 during 2019 and 2018, respectively, for research expenditures made during 2019 and 2018. If our subsidiary loses its ability to operate in Australia, or if we are ineligible or unable to receive the R&D incentive payment, or the Australian government significantly reduces or eliminates the incentive program, our business and results of operations may be adversely affected.
Fluctuations in insurance cost and availability could adversely affect our operating results or risk management profile.
We hold a number of insurance policies, including product liability insurance, directors’ and officers’ liability insurance, property insurance, and workers’ compensation insurance. The costs of maintaining adequate insurance coverage, most notably directors’ and officers’, have increased significantly recently and may continue to do so in the future, thereby adversely affecting our operating results. If such costs continue to increase, we may be forced to accept lower coverage and higher deductibles, which would have an adverse effect on our risk management profile and inhibit our ability to recruit qualified directors and officers. In addition, if any of our current insurance coverage should become unavailable to us or become economically impractical, we would be required to operate our business without indemnity from commercial insurance providers.
Risks Related to Intellectual Property
If we are unable to adequately protect and enforce our intellectual property, our competitors may take advantage of our development efforts or acquired technology and compromise our prospects of marketing and selling our product candidates.
We believe that patents and other proprietary rights are key to our business. Our policy is to file patent applications to protect technology, inventions, and improvements that may be important to the development of our business. We also rely upon trade secrets, know-how, continuing technological innovations, and licensing opportunities to develop and maintain our competitive position. We plan to enforce our issued patents and our rights to proprietary information and technology. We review third-party patents and patent applications, both to refine our own patent strategy and to identify useful licensing opportunities.
Our success depends, in part, on our ability to secure and protect our intellectual property rights and to operate without infringing on the proprietary rights of others or having third parties circumvent the rights owned or licensed by us. We have a number of patents, patent applications and rights to patents related to our compounds, product candidates and technology, but we cannot be certain that they will be enforceable or provide adequate protection or that pending patent applications will result in issued patents.
To the extent that development, manufacturing, and testing of our product candidates is performed by third party contractors, such work is performed pursuant to fee for service contracts. Under the contracts, all intellectual property, technology know-how, and trade secrets arising under such agreements are our exclusive property and must be kept confidential by the contractors. It is not possible for us to be certain that we have obtained from the contractors all necessary rights to such technologies. Disputes may arise as to the scope of the contract or possible breach of contract. No assurance can be given that our contracts would be enforceable or would be upheld by a court.
The patent positions of pharmaceutical and biotechnology firms, ourselves included, are uncertain and involve complex questions of law and fact for which important legal issues remain unresolved. Therefore, it is not clear whether our pending patent applications will result in the issuance of patents or whether we will develop additional proprietary products which are patentable. Part of our strategy is based on our ability to secure a patent position to protect our technology. There is no assurance that we will be successful in this approach and failure to secure patent protection may have a material adverse effect upon us and our financial condition. Also, we may fail in our attempt to commercialize products using currently patented or licensed technology without having to license additional patents. Moreover, it is not clear whether the patents issued or to be issued will provide us with any competitive advantages or if any such patents will be the target of challenges by third parties, whether the patents of others will interfere with our ability to market our products, or whether third parties will circumvent our patents by means of alternate processes. Furthermore, it is possible for others to develop products that have the same effect as our product candidates or technologies on an independent basis or to design around technologies patented by us. Patent applications relating to or affecting our business may have been filed by pharmaceutical or biotechnology companies or academic institutions. Such applications may conflict with our technologies or patent applications and such conflict could reduce the scope of patent protection that we could otherwise obtain or even lead to the rejection of our patent applications. There is no assurance that we can enter into licensing arrangements on commercially reasonable terms or develop or obtain alternative technology in respect of patents issued to third parties that incidentally cover our products or production technologies. Any inability to secure licenses or alternative technology could result in delays in the introduction of some of our product candidates or even lead to us being prevented from pursuing the development, manufacture or sale of certain products. Moreover, we could potentially incur substantial legal costs in defending legal actions that allege patent infringement, or by initiating patent infringement suits against others. It is not possible for us to be certain that we are the creator of inventions covered by pending patent applications or that we were the first to invent or file patent applications for any such inventions. While we have used commercially reasonable efforts to obtain assignments of intellectual property from all individuals who may have created materials on our behalf (including with respect to inventions covered by our patent and pending patent applications), it is not possible for us to be certain that we have obtained all necessary rights to such materials. No assurance can be given that our patents, if issued, would be upheld by a court, or that a competitor’s technology or product would be found to infringe on our patents. Moreover, much of our technology know-how that is not patentable may constitute trade secrets. Therefore, we require our employees, consultants, advisors and collaborators to enter into confidentiality agreements either as stand-alone agreements or as part of their employment or consulting contracts. However, no assurance can be given that such agreements will provide meaningful protection of our trade secrets, know-how or other proprietary information in the event of any unauthorized use or disclosure of confidential information. Also, while we have used commercially reasonable efforts to obtain executed copies of such agreements from all employees, consultants, advisors and collaborators, no assurance can be given that executed copies of all such agreements have been obtained.
We may require additional third-party licenses to effectively develop and manufacture our product candidates and are currently unable to predict the availability or cost of such licenses.
A substantial number of patents have already been issued to other biotechnology and pharmaceutical companies. To the extent that valid third-party patent rights cover our product candidates, we or our strategic collaborators would be required to seek licenses from the holders of these patents in order to manufacture, use, or sell these product candidates, and payments under them would reduce our profits from these product candidates. We are currently unable to predict the extent to which we may wish or be required to acquire rights under such patents, the availability and cost of acquiring such rights, and whether a license to such patents will be available on acceptable terms, or at all. There may be patents in the United States or in foreign countries or patents issued in the future that are unavailable to license on acceptable terms. Our inability to obtain such licenses may hinder or eliminate our ability to develop, manufacture and market our product candidates.
Changes in patent law and its interpretation could diminish the value of patents in general, thereby impairing our ability to protect our product candidates.
As is the case with other biotechnology and pharmaceutical companies, our success is heavily dependent on intellectual property rights, particularly patents. Obtaining and enforcing patents in the biopharmaceutical industry involves technological and legal complexity, and obtaining and enforcing biopharmaceutical patents is costly, time consuming, and inherently uncertain. The U.S. Supreme Court has ruled on several patent cases in recent years, either narrowing the scope of patent protection available in certain circumstances or weakening the rights of patent owners in certain situations. In addition to increasing uncertainty with regard to our and our licensors’ or collaborators’ ability to obtain patents in the future, this combination of events has created uncertainty with respect to the value of patents once obtained. Depending on decisions by the U.S. Congress, the federal courts, and the U.S. Patent and Trademark Office (USPTO), the laws and regulations governing patents could change in unpredictable ways that would weaken our and our licensors’ or collaborators’ ability to obtain new patents or to enforce existing patents and patents we and our licensors or collaborators may obtain in the future. Changes in either the patent laws or interpretation of the patent laws in the United States or other countries could increase the uncertainties and costs surrounding the prosecution of patent applications and the enforcement or defense of issued patents.
Assuming that other requirements for patentability are met, prior to March 2013, in the United States, the first to invent the claimed invention was entitled to the patent, while outside the United States, the first to file a patent application was entitled to the patent. After March 2013, under the Leahy-Smith America Invents Act, or the America Invents Act, enacted in September 2011, the United States transitioned to a first inventor to file system in which, assuming that other requirements for patentability are met, the first inventor to file a patent application will be entitled to the patent on an invention regardless of whether a third party was the first to invent the claimed invention. A third party that files a patent application in the USPTO after March 2013, but before us could, therefore, be awarded a patent covering an invention of ours even if we had made the invention before it was made by such third party. This will require us to be cognizant of the time from invention to filing of a patent application. Since patent applications in the United States and most other countries are confidential for a period of time after filing or until issuance, we cannot be certain that we or our licensors were the first to either (i) file any patent application related to our product candidates or (ii) invent any of the inventions claimed in our or our licensor’s patents or patent applications.
The America Invents Act also includes a number of significant changes that affect the way patent applications will be prosecuted and also may affect patent litigation. These include allowing third party submission of prior art to the USPTO during patent prosecution and additional procedures to attack the validity of a patent in USPTO-administered post-grant proceedings, including post-grant review, inter partes review, and derivation proceedings. Because of a lower evidentiary standard in USPTO proceedings compared to the evidentiary standard in United States federal courts necessary to invalidate a patent claim, a third party could potentially provide evidence in a USPTO proceeding sufficient for the USPTO to hold a claim invalid even though the same evidence would be insufficient to invalidate the claim if first presented in a district court action. Accordingly, a third party may attempt to use the USPTO procedures to invalidate our patent claims that would not have been invalidated if first challenged by the third party as a defendant in a district court action. Therefore, the America Invents Act and its implementation could increase the uncertainties and costs surrounding the prosecution of our owned or in-licensed patent applications and the enforcement or defense of our owned or in-licensed issued patents, all of which could have a material adverse effect on our business, financial condition, results of operations, and prospects.
The U.S. Supreme Court has ruled on several patent cases in recent years, either narrowing the scope of patent protection available in certain circumstances or weakening the rights of patent owners in certain situations. In addition to increasing uncertainty with regard to our and our licensors’ or collaborators’ ability to obtain patents in the future, this combination of events has created uncertainty with respect to the value of patents, once obtained. Depending on decisions by the U.S. Congress, the federal courts, and the U.S. Patent and Trademark Office, and similar legislative, judicial, and administrative bodies in other countries, the laws and regulations governing patents could change in unpredictable ways that would weaken our and our licensors’ or collaborators’ ability to obtain new patents or to enforce existing patents and patents we and our licensors or collaborators may obtain in the future.
Litigation regarding patents, patent applications, and other proprietary rights may be expensive, time consuming and cause delays in the development and manufacturing of our product candidates.
Third parties may claim that we are using their proprietary information without authorization. Third parties may also have or obtain patents and may claim that technologies licensed to or used by us infringe their patents. If we are required to defend patent infringement actions brought by third parties, or if we sue to protect our own patent rights or otherwise to protect our proprietary information and to prevent its disclosure, we may be required to pay substantial litigation costs and managerial attention may be diverted from business operations even if the outcome is in our favor. In addition, any legal action that seeks damages or an injunction to stop us from carrying on our commercial activities relating to the affected technologies could subject us to monetary liability (including treble damages and attorneys’ fees if we are found to have willfully infringed) and require us or any third-party licensors to obtain a license to continue to use the affected technologies. We cannot predict whether we would prevail in any of these types of actions or that any required license would be available on commercially acceptable terms or at all. Some of our competitors may be able to sustain the costs of complex patent litigation more effectively than we can because they have substantially greater resources.
Competitors may infringe our patents or other intellectual property. If we were to initiate legal proceedings against a third party to enforce a patent covering our product candidates, the defendant could counterclaim that the patent covering our product candidate is invalid and/or unenforceable. In patent litigation in the United States, defendant counterclaims alleging invalidity and/or unenforceability are commonplace. Grounds for a validity challenge could be an alleged failure to meet any of several statutory requirements, including lack of novelty, obviousness, written description or non-enablement. Grounds for an unenforceability assertion could be an allegation that someone connected with prosecution of the patent withheld relevant information from the USPTO, or made a misleading statement, during prosecution. The outcome following legal assertions of invalidity and unenforceability is unpredictable. Moreover, similar challenges may be made by third parties outside the context of litigation, e.g., via administrative proceedings such as post grant or inter partes review in the United States or via oppositions or other similar proceedings in other countries/regions.
Interference or derivation proceedings provoked by third parties or brought by us or declared by the USPTO may be necessary to determine the priority of inventions with respect to our patents or patent applications. An unfavorable outcome could require us to cease using the related technology or to attempt to license rights to it from the prevailing party. Our business could be harmed if the prevailing party does not offer us a license on commercially reasonable terms or at all, or if a non-exclusive license is offered and our competitors gain access to the same technology. Our defense of litigation, validity or enforceability, interference or derivation proceedings may fail and, even if successful, may result in substantial costs and distract our management and other employees. In addition, the uncertainties associated with litigation or such other proceedings could have a material adverse effect on our ability to raise the funds necessary to continue our clinical trials, continue our research programs, license necessary technology from third parties, or enter into development partnerships that would help us bring our product candidates to market.
Furthermore, because of the substantial amount of discovery required in connection with intellectual property litigation or administrative proceedings, there is a risk that some of our confidential information could be compromised by disclosure. There could also be public announcements of the results of hearings, motions, or other interim proceedings or developments. If securities analysts or investors perceive these results to be negative, it could have a material adverse effect on the market price of our common shares.
If we fail to comply with our obligations in the agreements under which we license intellectual property rights from third parties or otherwise experience disruptions to our business relationships with our licensors, we could lose intellectual property rights that are important to our business.
We are a party to a license agreement relating to an expression system and cell line for use in the production of DM199 or any human KLK1, and we may need to obtain additional licenses from others to advance our R&D activities or allow the commercialization of DM199 or any other product candidates we may identify and pursue. Future license agreements may impose various development, diligence, commercialization and other obligations on us. If any of our in-licenses are terminated, or if the underlying patents fail to provide the intended exclusivity, competitors or other third parties may gain access to technologies that are material to our business, and we may be required to cease our development and commercialization of DM199 or other product candidates that we may identify or to seek alternative manufacturing methods. However, suitable alternatives may not be available or the development of suitable alternatives may result in a significant delay in our commercialization of DM199. Any of the foregoing could have a material adverse effect on our competitive position, business, financial condition, results of operations and prospects.
Moreover, disputes may arise regarding intellectual property subject to a licensing agreement, including, among others:
|
● |
the scope of rights granted under the license agreement and other interpretation-related issues; |
|
● |
the extent to which our product candidates, technology and processes infringe on intellectual property of the licensor that is not subject to the licensing agreement; |
|
● |
the sublicensing of patent and other rights under our collaborative development relationships; |
|
● |
our diligence obligations under the license agreement and what activities satisfy those diligence obligations; |
|
● |
the inventorship and ownership of inventions and know-how resulting from the joint creation or use of intellectual property by our licensors and us and our partners; and |
|
● |
the priority of invention of patented technology. |
In addition, the agreements under which we currently license intellectual property or technology from third parties are complex, and certain provisions in such agreements may be susceptible to multiple interpretations. The resolution of any contract interpretation disagreement that may arise could narrow what we believe to be the scope of our rights to the relevant intellectual property or technology, or increase what we believe to be our financial or other obligations under the relevant agreement, either of which could have a material adverse effect on our business, financial condition, results of operations, and prospects. Moreover, if disputes over intellectual property that we have licensed prevent or impair our ability to maintain our current licensing arrangements on commercially acceptable terms, we may be unable to successfully develop and commercialize the affected product candidates, which could have a material adverse effect on our business, financial condition, results of operations, and prospects.
Our reliance on third parties requires us to share our trade secrets, which increases the possibility that a competitor will discover them.
Because we rely on third parties to develop our products, we must share trade secrets with them. We seek to protect our proprietary technology in part by entering into confidentiality agreements and, if applicable, material transfer agreements, collaborative research agreements, employment or consulting agreements, or other similar agreements with our collaborators, advisors, employees, and consultants prior to beginning research or disclosing proprietary information. These agreements typically restrict the ability of our collaborators, advisors, employees, and consultants to publish data potentially relating to our trade secrets. Our academic collaborators typically have rights to publish data, provided that we are notified in advance and may delay publication for a specified time in order to secure our intellectual property rights arising from the collaboration. In other cases, publication rights are controlled exclusively by us, although in some cases we may share these rights with other parties. We also conduct joint R&D programs which may require us to share trade secrets under the terms of R&D collaboration or similar agreements. However, we cannot be certain that such agreements have been entered into with all relevant parties. Moreover, despite our efforts to protect our trade secrets, our competitors may discover our trade secrets, either through breach of these agreements, independent development, or publication of information including our trade secrets in cases where we do not have proprietary or otherwise protected rights at the time of publication. Trade secrets can be difficult to protect. If the steps taken to maintain our trade secrets are deemed inadequate, we may have insufficient recourse against third parties for misappropriating any trade secrets. A competitor’s discovery of our trade secrets may impair our competitive position and could have a material adverse effect on our business and financial condition.
Patent terms may be inadequate to protect our competitive position on our product candidates for an adequate amount of time.
Patents have a limited lifespan. In the United States, if all maintenance fees are timely paid, the natural expiration of a patent is generally 20 years from its earliest U.S. non-provisional filing date. Various extensions may be available, but the life of a patent, and the protection it affords, is limited. Even if patents covering our product candidates are obtained, once the patent life has expired, we may be open to competition from competitive products, including generics or biosimilars. Given the amount of time required for the development, testing and regulatory review of new product candidates, patents protecting such candidates might expire before or shortly after such candidates are commercialized. As a result, our owned and licensed patent portfolio may not provide us with sufficient rights to exclude others from commercializing products similar or identical to ours.
We may be subject to claims that our employees, consultants or independent contractors have wrongfully used or disclosed confidential information of third parties or that our employees have wrongfully used or disclosed alleged trade secrets of their former employers.
As is common in the biotechnology and pharmaceutical industry, we employ individuals who were previously employed at universities or other biotechnology or pharmaceutical companies, including our competitors or potential competitors. Although we try to ensure that our employees, consultants and independent contractors do not use the proprietary information or know-how of others in their work for us, we may be subject to claims that we or our employees, consultants or independent contractors have inadvertently or otherwise used or disclosed intellectual property, including trade secrets or other proprietary information, of any of our employees’ former employer or other third parties. Litigation may be necessary to defend against these claims. If we fail in defending any such claims, in addition to paying monetary damages, we may lose valuable intellectual property rights or personnel, which could adversely impact our business. Even if we are successful in defending against such claims, litigation could result in substantial costs and be a distraction to management and other employees.
Obtaining and maintaining our patent protection depends on compliance with various procedural, document submission, fee payment and other requirements imposed by governmental patent agencies, and our patent protection could be reduced or eliminated for non-compliance with these requirements.
Periodic maintenance fees, renewal fees, annuity fees and various other governmental fees on patents and/or applications will be due to be paid to the USPTO and various governmental patent agencies outside of the United States in several stages over the lifetime of the patents and/or applications. We have systems in place to remind us to pay these fees, and we employ an outside firm and rely on our outside counsel to pay these fees due to non-U.S. patent agencies. The USPTO and various non-U.S. governmental patent agencies require compliance with a number of procedural, documentary, fee payment and other similar provisions during the patent application process. We employ reputable law firms and other professionals to help us comply, and in many cases, an inadvertent lapse can be cured by payment of a late fee or by other means in accordance with the applicable rules. However, there are situations in which non-compliance can result in abandonment or lapse of the patent or patent application, resulting in partial or complete loss of patent rights in the relevant jurisdiction. In such an event, our competitors might be able to enter the market and this circumstance would have a material adverse effect on our business.
We may not be able to protect our intellectual property rights throughout the world.
Filing, prosecuting and defending patents on our product candidates in all countries throughout the world would be prohibitively expensive, and our intellectual property rights in some countries outside the United States can be less extensive than those in the United States. In addition, the laws of some foreign countries do not protect intellectual property rights to the same extent as federal and state laws in the United States. Consequently, we may not be able to prevent third parties from practicing our inventions in all countries outside the United States, or from selling or importing products made using our inventions in and into the United States or other jurisdictions. Competitors may use our technologies in jurisdictions where we have not obtained patent protection to develop their own products and may also export infringing products to territories where we have patent protection, but enforcement is not as strong as that in the United States. These products may compete with our products and our patents or other intellectual property rights may not be effective or sufficient to prevent them from competing.
Many companies have encountered significant problems in protecting and defending intellectual property rights in foreign jurisdictions. The legal systems of certain countries, particularly certain developing countries, do not favor the enforcement of patents, trade secrets, and other intellectual property protection, particularly those relating to biotechnology products, which could make it difficult for us to stop the infringement of our patents or marketing of competing products in violation of our proprietary rights generally. Proceedings to enforce our patent rights in foreign jurisdictions, whether or not successful, could result in substantial costs and divert our efforts and attention from other aspects of our business, could put our patents at risk of being invalidated or interpreted narrowly and could put our patent applications at risk of not issuing and could provoke third parties to assert claims against us. We may not prevail in any lawsuits that we initiate and the damages or other remedies awarded, if any, may not be commercially meaningful. Accordingly, our efforts to enforce our intellectual property rights around the world may be inadequate to obtain a significant commercial advantage from the intellectual property that we develop or license.
Risks Related to Our Common Shares
Our common share price has been volatile and may continue to be volatile.
Our common shares trade on The Nasdaq Capital Market under the trading symbol “DMAC.” A number of factors could influence the volatility in the trading price of our common shares, including changes in the economy or in the financial markets, industry related developments, and the impact of material events and changes in our operations. Our quarterly losses may vary because of expenses we incur related to our R&D and clinical activities, including the timing of costs for manufacturing DM199 and initiating and completing preclinical and clinical trials. Each of these factors could lead to increased volatility in the market price of our common shares. In addition, the market prices of the securities of our competitors may also lead to fluctuations in the trading price of our common shares.
We do not have a very active trading market for our common shares and one may never develop.
Our common shares commenced trading in the United States on The Nasdaq Capital Market in December 2018. Previously our shares traded in Canada on the TSX Venture Exchange. We do not have a very active trading market for our common shares, and one may never develop. Although we anticipate a more active trading market for our common shares will develop in the future, we can give no assurance that this will occur or that an active trading market will be sustained. If an active market for our common shares does not develop, it may be difficult for you to sell our common shares at a favorable price or at all.
We may issue additional common shares resulting in share ownership dilution.
Future dilution will likely occur due to anticipated future equity issuances by us. To the extent we raise additional capital through the sale of equity or convertible debt securities, the ownership interests of our shareholders will be diluted. In addition, as of December 31, 2019, we had outstanding warrants to purchase 971,953 common shares, options to purchase 1,220,359 common shares, deferred share units representing 21,183 common shares and 1,384,822 common shares reserved for future issuance in connection with future grants under the DiaMedica Therapeutics Inc. 2019 Omnibus Incentive Plan. If these or any future outstanding warrants, options, or deferred share units are exercised or otherwise converted into our common shares, our shareholders will experience additional dilution.
If there are substantial sales of our common shares or the perception that such sales could occur, the market price of our common shares could decline.
Sales of substantial numbers of our common shares or the perception that such sales could occur could cause a decline in the market price of our common shares. Any sales by existing shareholders or holders who exercise their warrants or stock options may have an adverse effect on our ability to raise capital and may adversely affect the market price of our common shares.
We could be subject to securities class action litigation, which is expensive and could divert management attention.
In the past, securities class action litigation has often been brought against a company following a decline or increase in the market price of its securities or certain significant business transactions. We may become involved in this type of litigation in the future, especially if our clinical trial results are not successful or we enter into an agreement for a significant business transaction. If we face such litigation, it could result in substantial costs and a diversion of management’s attention and our resources, which could harm our business. This is particularly true in light of our limited securities litigation insurance coverage.
If securities or industry analysts do not publish research or reports about our business, or publish negative reports about our business, the market price of our common shares and trading volume could decline.
The market price and trading volume for our common shares will depend in part on the research and reports that securities or industry analysts publish about us or our business. We do not have any control over these analysts. There can be no assurance that analysts will continue to cover us or provide favorable coverage. If one or more of the analysts who cover us downgrade our common shares or change their opinion of our common shares, the market price of our common shares would likely decline. If one or more of these analysts cease coverage of our company or fail to regularly publish reports on us, we could lose visibility in the financial markets, which could cause the market price of our common shares or trading volume to decline.
We are an “emerging growth company” and a “smaller reporting company,” and the reduced disclosure requirements applicable to us as such may make our common shares less attractive to our shareholders and investors.
We are an “emerging growth company,” as defined in the Jumpstart Our Business Startups Act of 2012. We may remain an emerging growth company until December 31, 2023, the last day of the fiscal year following the fifth anniversary of our first sale of common shares pursuant to a registration statement under the Securities Act of 1933, as amended (the Securities Act) or until such earlier time as we have more than $1.07 billion in annual revenue, the market value of our common shares held by non-affiliates is more than $700 million or we issue more than $1 billion of non-convertible debt over a three-year period. For so long as we remain an emerging growth company, we are permitted and intend to rely on exemptions from certain disclosure requirements that are applicable to other public companies that are not emerging growth companies. These exemptions include not being required to comply with the auditor attestation requirements of Section 404 of the Sarbanes-Oxley Act of 2002 (Section 404), not being required to comply with any requirement that may be adopted by the Public Company Accounting Oversight Board regarding mandatory audit firm rotation or a supplement to the auditor’s report providing additional information about the audit and the financial statements, reduced disclosure obligations regarding executive compensation and exemptions from the requirements of holding a non-binding advisory vote on executive compensation and shareholder approval of any golden parachute payments not previously approved.
We are also a “smaller reporting company” under the federal securities laws and, as such, are subject to scaled disclosure requirements afforded to such companies. For example, as a smaller reporting company, we are subject to reduced executive compensation disclosure requirements.
Our shareholders and investors may find our common shares less attractive as a result of our status as an “emerging growth company” and “smaller reporting company” and our reliance on the reduced disclosure requirements afforded to these companies. If some of our shareholders or investors find our common shares less attractive as a result, there may be a less active trading market for our common shares and the market price of our common shares may be more volatile.
Our inability to comply with Nasdaq’s continued listing requirements could result in our common shares being delisted, which could affect the market price and liquidity of our common shares and reduce our ability to raise capital.
Because our common shares are listed on The Nasdaq Capital Market, we are required to meet certain qualitative and financial tests to maintain the listing of our common shares on The Nasdaq Capital Market. If we do not maintain compliance with Nasdaq’s continued listing requirements within specified periods and subject to permitted extensions, our common shares may be recommended for delisting (subject to any appeal we would file). No assurance can be provided that we will comply with these continued listing requirements. If our common shares were delisted, it could be more difficult to buy or sell our common shares and to obtain accurate quotations, and the price of our common shares could suffer a material decline. Delisting would also impair our ability to raise additional capital.
Any failure to maintain an effective system of internal controls may result in material misstatements of our consolidated financial statements or cause us to fail to meet our reporting obligations or fail to prevent fraud; and in that case, our shareholders or other investors could lose confidence in our financial reporting, which would harm our business and could negatively impact the market price of our common shares.
Effective internal controls are necessary for us to provide reliable financial reports and prevent fraud. If we fail to maintain an effective system of internal controls, we might not be able to report our financial results accurately or prevent fraud; and in that case, our shareholders or other investors could lose confidence in our financial reporting, which would harm our business and could negatively impact the market price of our common shares. As a result of our limited administrative staffing levels, internal controls that rely on segregation of duties in many cases are not possible. Due to resource constraints and the present stage of our development, we do not have sufficient size and scale to warrant the hiring of additional staff to address this potential weakness at this time. To help mitigate the impact of this, we are highly reliant on the performance of compensating procedures and senior management’s review and approval. Even if we conclude that our internal control over financial reporting provides reasonable assurance regarding the reliability of financial reporting and the preparation of consolidated financial statements for external purposes in accordance with generally accepted accounting principles in the United States, because of its inherent limitations, internal control over financial reporting may not prevent or detect fraud or misstatements. Failure to implement required new or improved controls, or difficulties encountered in their implementation, could harm our results of operations or cause us to fail to meet our future reporting obligations.
If we fail to timely achieve and maintain the adequacy of our internal control over financial reporting, we may not be able to produce reliable financial reports or help prevent fraud. Our failure to achieve and maintain effective internal control over financial reporting could prevent us from complying with our reporting obligations on a timely basis, which could result in the loss of shareholder or other investor confidence in the reliability of our consolidated financial statements, harm our business and negatively impact the market price of our common shares.
Pursuant to Section 404 of the Sarbanes-Oxley Act, we are required to furnish a report by our management regarding our internal control over financial reporting, and if we become an accelerated filer under the federal securities laws, we will be required to include an attestation report on internal control over financial reporting issued by our independent registered public accounting firm. There is a risk that neither we nor our independent registered public accounting firm will be able to conclude within the prescribed timeframe that our internal control over financial reporting is effective as required by Section 404. This could result in an adverse reaction in the financial markets due to a loss of confidence in the reliability of our financial statements.
We have never paid dividends and do not expect to do so in the foreseeable future.
We have not declared or paid any cash dividends on our common shares to date. The payment of dividends in the future will be dependent on our earnings and financial condition and on such other factors as our Board of Directors considers appropriate. Unless and until we pay dividends, shareholders may not receive a return on their common shares. There is no present intention by our Board of Directors to pay dividends on our common shares. We currently intend to retain all of our future earnings, if any, to finance the growth and development of our business. In addition, the terms of any future debt agreements may preclude us from paying dividends. As a result, appreciation, if any, in the market price of our common shares will be your sole source of gain for the foreseeable future.
Risks Related to Our Jurisdiction of Organization
It may be difficult for non-Canadian shareholders or investors to obtain and enforce judgments against us because of our organization as a British Columbia corporation.
We are a corporation existing under the laws of British Columbia, Canada. Two of our directors are residents of Canada, and all or a substantial portion of their assets, and a portion of our assets, are located outside the United States. Consequently, it may be difficult for holders of our securities who reside in the United States to effect service within the United States upon those directors who are not residents of the United States. It may also be difficult for holders of our securities who reside in the United States to realize in the United States upon judgments of courts of the United States predicated upon our civil liability and the civil liability of our directors, and officers under the United States federal securities laws. Our shareholders and other investors should not assume that British Columbian or Canadian courts (i) would enforce judgments of United States courts obtained in actions against us or such directors, or officers predicated upon the civil liability provisions of the United States federal securities laws or the securities or “blue sky” laws of any state or jurisdiction of the United States, or (ii) would enforce, in original actions, liabilities against us or such directors, or officers predicated upon the United States federal securities laws or any securities or “blue sky” laws of any state or jurisdiction of the United States. In addition, the protections afforded by the securities laws of British Columbia or Canada may not be available to our shareholders or other investors in the United States.
We are governed by the corporate laws of British Columbia, which in some cases have a different effect on shareholders than the corporate laws in effect in the United States.
We are a British Columbia corporation. Our corporate affairs and the rights of holders of our common shares are governed by British Columbia’s Business Corporations Act and applicable securities laws, which laws may differ from those governing a company formed under the laws of a United States jurisdiction. The provisions under the BCBCA and other relevant laws may affect the rights of shareholders differently than those of a company governed by the laws of a United States jurisdiction and may, together with our Notice of Articles and Articles, have the effect of delaying, deferring or discouraging another party from acquiring control of our company by means of a tender offer, proxy contest or otherwise, or may affect the price an acquiring party would be willing to offer in such an instance. The material differences between the BCBCA and the Delaware General Corporation Law, by way of example, that may be of most interest to shareholders include the following:
|
● |
for material corporate transactions (such as mergers and amalgamations, other extraordinary corporate transactions, or amendments to our Notice of Articles), the BCBCA, subject to the provisions of our Articles, generally requires two-thirds majority vote by shareholders; whereas, the DGCL generally only requires a majority vote of shareholders; |
|
● |
under the BCBCA, a holder of 5% or more of our common shares can requisition a special meeting at which any matters that can be voted on at our annual meeting can be considered; whereas, the DGCL does not give this right; |
|
● |
our Articles require two-thirds majority vote by shareholders to pass a resolution for one or more directors to be removed; whereas, the DGCL only requires the affirmative vote of a majority of the shareholders; and |
|
● |
our Articles may be amended by resolution of our directors to alter our authorized share structure, including to (a) subdivide or consolidate any of our shares and (b) create additional classes or series of shares; whereas, under the DGCL, a majority vote by shareholders is generally required to amend a corporation’s certificate of incorporation and a separate class vote may be required to authorize alternations to a corporation’s authorized share structure. |
We cannot predict if investors find our common shares less attractive because of these material differences. If some investors find our common shares less attractive as a result, there may be a less active trading market for our common shares and our share price may be more volatile.
Our shareholder rights plan may delay or prevent an acquisition of us that shareholders may consider favorable or may prevent efforts by our shareholders to change our directors or our management, which could decrease the value of our common shares.
On December 21, 2017, our shareholders approved the renewal of a shareholder rights plan agreement through the annual general meeting to be held by DiaMedica in 2020. The shareholder rights plan is designed to provide adequate time for our Board of Directors and shareholders to assess an unsolicited takeover bid for our company, to provide our Board of Directors with sufficient time to explore and develop alternatives for maximizing shareholder value if a takeover bid is made, and to provide shareholders with an equal opportunity to participate in a takeover bid and receive full and fair value for their common shares. Under the terms of the shareholder rights plan, the rights will become exercisable only when a person, including any party related to it, acquires or attempts to acquire 20% or more of our outstanding common shares without complying with the “permitted bid” provisions of the plan or without approval of our Board of Directors. Should such an acquisition occur or be announced, each right would, upon exercise, entitle a rights holder, other than the acquiring person and related persons, to purchase common shares at a 50% discount to the market price at the time. Under the plan, a “permitted bid” is a bid made to all holders of our common shares and which is open for acceptance for not less than 60 days. If at the end of 60 days at least 50% of the outstanding common shares, other than those owned by the offeror and certain related parties have been tendered, the offeror may take up and pay for the common shares but must extend the bid for a further 10 days to allow other shareholders to tender.
While we believe our rights plan enables our Board of Directors to help ensure that our shareholders are not deprived of the opportunity to realize the full and fair value of their investments, the rights plan may inhibit a change in control of our company by a third party in a transaction not approved by our Board of Directors. If a change in control is inhibited or delayed in this manner, it may adversely affect the market price of our common shares. The shareholder rights plan is set to expire at the close of our annual general meeting of shareholders in 2020 and we currently anticipate letting the plan expire at that time.
We may be classified as a “passive foreign investment company” in future taxable years, which may have adverse U.S. federal income tax consequences for U.S. shareholders.
Generally, for any taxable year in which 75% or more of our gross income is passive income, or at least 50% of the average quarterly value of our assets (which may be determined in part by the market value of our common shares, which is subject to change) are held for the production of, or produce, passive income, we would be characterized as a passive foreign investment company (PFIC) for U.S. federal income tax purposes. The average percentage of a corporation’s assets that produce or are held for the production of passive income generally is determined on the basis of the fair market value of the corporation’s assets at the end of each quarter (which may be determined in part by the market value of our common shares, which is subject to change).
The tests for determining PFIC status for any taxable year are dependent upon a number of factors, some of which are beyond our control, including the value of our assets, the market price of our common shares, and the amount and type of our gross income. Based on these tests (i) we believe that we were a PFIC for the taxable year ended December 31, 2016, and (ii) we do not believe that we were a PFIC for the taxable years ended December 31, 2019, 2018 and 2017. Our status as a PFIC is a fact-intensive determination made for each taxable year, and we cannot provide any assurance regarding our PFIC status for the taxable year ending December 31, 2020 or for future taxable years. U.S. shareholders who own our common shares for any period during which we are a PFIC will be required to file IRS Form 8621 for each tax year during which they hold our common shares.
If we are a PFIC for any year during a non-corporate U.S. shareholder’s holding period of our common shares, and the U.S. shareholder does not make a Qualified Electing Fund election (QEF Election) or a “mark-to-market” election, both as described below, then such non-corporate U.S. shareholder generally will be required to treat any gain realized upon a disposition of our common shares, or any so-called “excess distribution” received on our common shares, as ordinary income, rather than as capital gain, and the preferential tax rate applicable to dividends received on our common shares would not be available. This income generally would be allocated over a U.S. shareholder’s holding period with respect to our common shares and the amount allocated to prior years will be subject to tax at the highest tax rate in effect for that year and an interest charge would be imposed on the amount of deferred tax on the income allocated to prior taxable years. Pursuant to the specific provisions of the PFIC rules, a taxpayer may realize gain on the disposition of common shares if the securities are disposed of by a holder whose securities are attributed to the U.S. shareholder, if the securities are pledged as security for a loan, transferred by gift or death, or are subject to certain corporate distributions. Additionally, if we are a PFIC, a U.S. shareholder who acquires our common shares from a decedent would be denied normally available step-up in tax basis for our common shares to fair market value at the date of death but instead would have a tax basis equal to the lower of the fair market value of such common shares or the decedent’s tax basis in such common shares.
A U.S. shareholder may avoid these adverse tax consequences by making a timely and effective QEF election. A U.S. shareholder who makes a QEF election generally must report, on a current basis, its share of our ordinary earnings and net capital gains, whether or not we distribute any amounts to our shareholders, and would be required to comply with specified information reporting requirements. Any gain subsequently recognized upon the sale by that U.S. shareholder of the common shares generally would be taxed as capital gain and the denial of the basis step-up at death described above would not apply. The QEF election is available only if the company characterized as a PFIC provides a U.S. shareholder with certain information regarding its earnings and capital gains, as required under applicable U.S. Treasury regulations. We intend to provide all information and documentation that a U.S. shareholder making a QEF election is required to obtain for U.S. federal income tax purposes (e.g., the U.S. shareholder’s pro rata share of ordinary income and net capital gain, and a “PFIC Annual Information Statement” as described in applicable U.S. Treasury regulations).
As an alternative to a QEF Election, a U.S. shareholder may also mitigate the adverse tax consequences of PFIC status by timely making a “mark-to-market” election. A U.S. shareholder who makes the mark-to-market election generally must include as ordinary income each year the increase in the fair market value of the common shares and deduct from gross income the decrease in the value of such shares during each of its taxable years. Losses would be allowed only to the extent of the net mark-to-market gain accrued under the election. If a mark-to-market election with respect to our common shares is in effect on the date of a U.S. shareholder’s death, the tax basis of the common shares in the hands of a U.S. shareholder who acquired them from a decedent will be the lesser of the decedent’s tax basis or the fair market value of the common shares. A mark-to-market election may be made and maintained only if our common shares are regularly traded on a qualified exchange, including Nasdaq. Whether our common shares are regularly traded on a qualified exchange is an annual determination based on facts that, in part, are beyond our control. Accordingly, a U.S. shareholder might not be eligible to make a mark-to-market election to mitigate the adverse tax consequences if we are characterized as a PFIC.
Certain economic risks are inherent in making either a QEF Election or a mark-to-market election. If a QEF Election is made, it is possible that a small but significant amount of earned income will be reported to a U.S. shareholder as taxable income as long as the company invests its cash reserves, and income taxes will be due and payable on such an amount. A U.S. shareholder of our common shares may pay tax on such “phantom” income, i.e., income reported to it pursuant to the QEF Election, but not actually received. There is no assurance that any distribution or profitable sale will ever be made regarding our common shares, so the tax liability may result in a net economic loss. A mark-to-market election may result in significant share price gains in one year causing a significant income tax liability. This gain may be offset in another year by significant losses. If a mark-to-market election is made, this highly variable tax gain or loss may result in substantial and unpredictable changes in taxable income. The amount included in income under a mark-to-market election may be substantially greater than the amount included under a QEF election. Both the QEF and mark-to-market elections are binding on the U.S. shareholder for all subsequent years that the U.S. shareholder owns our shares unless permission to revoke the election is granted by the IRS.
Although we generally will continue to be treated as a PFIC as to any U.S. shareholder if we are a PFIC for any year during a U.S. shareholder’s holding period, if we cease to satisfy the requirements for PFIC classification, the U.S. shareholder may avoid PFIC classification for subsequent years if the U.S. shareholder elects to make a so-called “purging election,” by recognizing income based on the unrealized appreciation in the common shares through the close of the tax year in which we cease to be a PFIC.
RULES RELATING TO A PFIC ARE VERY COMPLEX. YOU SHOULD CONSULT YOUR TAX ADVISER CONCERNING THE RELATIVE MERITS AND THE ECONOMIC AND TAX IMPACT OF PFIC RULES TO YOUR INVESTMENT IN OUR COMMON SHARES AS A NON-ELECTING U.S. SHAREHOLDER, A U.S. SHAREHOLDER MAKING A QEF ELECTION, OR A U.S. SHAREHOLDER MAKING A MARK-TO-MARKET ELECTION.
Should we be classified as a PFIC during a U.S. shareholder’s holding period for our common shares, each such U.S. shareholder should consult their own tax advisors with respect to the possibility of making these elections and the U.S. federal income tax consequences of the acquisition, ownership and disposition of our common shares. In addition, the possibility of us being classified as a PFIC may deter certain U.S. investors from purchasing our common shares, which could have an adverse impact on the market price of our common shares and our ability to raise additional financing by selling equity securities, including our common shares.
|
Item 1B. |
Unresolved Staff Comments |
This Item 1B is inapplicable to us as a smaller reporting company.
|
Item 2. |
Properties |
Our principal executive offices, together with our research and development operations, are at the office of our wholly owned subsidiary, DiaMedica USA Inc., located at Two Carlson Parkway, Suite 260, Minneapolis, Minnesota, USA 55447. We lease these premises, which consist of approximately 3,800 square feet, pursuant to a lease that expires in August 2022. We believe that our facilities are adequate for our current needs and that suitable additional space will be available as and when needed on acceptable terms.
|
Item 3. |
Legal Proceedings |
In March 2013, we entered into a clinical research agreement with PRA Netherlands to perform a double-blinded, placebo-controlled, single-dose and multiple-dose study to evaluate the safety, tolerability, pharmacokinetics, pharmacodynamics and proof of concept of DM199 in healthy subjects and in patients with Type 2 diabetes mellitus. In one arm of this study, we enrolled 36 patients with Type 2 diabetes who were treated with two SC dose levels of DM199 over a 28-day period. This study achieved its primary endpoint and demonstrated that DM199 was well-tolerated. The secondary endpoints for this study, however, were not met. The secondary efficacy endpoints were confounded due to what we believe were significant execution errors caused by protocol deviations occurring at the clinical trial site that were unable to be reconciled. To date, we have been unable to obtain the complete study records from PRA Netherlands and generate a final study report. On November 14, 2017, we initiated litigation with PRA Netherlands in the United States District Court, Southern District of New York, to compel them to comply with the terms of the clinical research agreement, including providing full study records and to recover damages. After PRA Netherlands objected to the venue, on August 24, 2018, we re-filed our complaint against both PRA Netherlands and its U.S. parent, PRA Health Sciences, Inc. (“PRA USA” and collectively with PRA Netherlands, PRA), in the United States District Court, District of Delaware. PRA again objected to the venue, we intend to re-file our complaint against PRA in the United States District Court, District of Minnesota. The complaint alleges, among other things, that PRA failed to conduct the study in accordance with the study protocol and with generally accepted standards for conducting such clinical trials and that PRA further refused to provide us with all data, records and documentation, and/or access thereto, related to the study in accordance with the clinical trial study agreement. The complaint seeks to compel PRA to comply with the terms of the clinical trial study agreement, including providing full study records and to recover damages. On November 19, 2018, PRA Netherlands and PRA USA filed motions to dismiss the lawsuit. We subsequently requested, and PRA Netherlands and PRA USA agreed, that we be permitted to file a motion seeking to transfer the Delaware action to the United States District Court, District of Minnesota. On February 20, 2019, we filed this motion to transfer venue.
From time to time, we may be subject to other various ongoing or threatened legal actions and proceedings, including those that arise in the ordinary course of business, which may include employment matters and breach of contract disputes. Such matters are subject to many uncertainties and to outcomes that are not predictable with assurance and that may not be known for extended periods of time. Other than the PRA matter noted above, we are not currently engaged in or aware of any threatened legal actions.
|
Item 4. |
Mine Safety Disclosures |
Not applicable.
PART II
|
Item 5. |
Market for Registrant’s Common Equity, Related Stockholder Matters and Issuer Purchases of Equity Securities |
Market Information
Our common shares are listed on The Nasdaq Capital Market under the trading symbol “DMAC” and have been so listed since December 7, 2018, the date of our initial public offering in the United States. Our common shares previously traded in Canada on the TSX Venture Exchange under the trading symbol “DMA” through January 18, 2019. We voluntarily delisted our common shares from the TSX Venture Exchange since we believe that the financial and administrative costs associated with maintaining a dual listing are not justified. Prior to our initial public offering, our common shares traded over-the-counter in the United States on the OTCQB marketplace under the trading symbol “DMCAD” from November 15, 2018 to December 7, 2018 and before November 15, 2018, under the trading symbol “DMCAF.”
Number of Record Holders
As of March 20, 2020, we had 43 holders of record of our common shares. This does not include persons whose common shares are in nominee or “street name” accounts through brokers or other nominees.
Dividend Policy
We have never declared or paid cash dividends on our common shares, and currently do not have any plans to do so in the foreseeable future. We expect to retain our future earnings, if any, for use in the operation and expansion of our business. Additionally, we may in the future become subject to contractual restrictions on, or prohibitions against, the payment of dividends. Subject to the foregoing, the payment of cash dividends in the future, if any, will be at the discretion of our Board of Directors and will depend upon such factors as earnings levels, capital requirements, our overall financial condition and any other factors deemed relevant by our Board of Directors. As a result, you will likely need to sell your common shares to realize a return on your investment and you may not be able to sell your shares at or above the price you paid for them.
Use of Proceeds
On December 11, 2018, the SEC declared effective our registration statement on Form S-1 (File No. 333- 228313), as amended, filed in connection with our initial public offering. Pursuant to the registration statement, we issued and sold an aggregate of 4,100,000 common shares in the initial public offering at a price to the public of $4.00 per share. As a result of the offering, we received gross proceeds of approximately $16.4 million, resulting in net proceeds to us of approximately $14.7 million, after deducting the underwriting discount and offering expenses. None of the expenses associated with the initial public offering were paid to directors, officers, persons owning ten percent or more of any class of equity securities, or to their associates, or to our affiliates. Craig-Hallum Capital Group LLC (Craig-Hallum) acted as the sole managing underwriter for the offering.
As of December 31, 2019, we have used approximately $9.1 million of the proceeds from our initial public offering to fund clinical development of DM199, to conduct research activities and for working capital and general corporate purposes. No payments were made by us to directors, officers or persons owning ten percent or more of our common shares or to their associates, or to our affiliates, other than payments in the ordinary course of business to officers for salaries and bonuses and to non-employee directors as compensation for board and board committee service. There has been no material change in the planned use of proceeds from our initial public offering from that described in the final prospectus, dated December 6, 2018, filed with the SEC on December 10, 2018 pursuant to Rule 424(b)(4) under the Securities Act.
Pending their use as described above, we have invested the net proceeds in short-term, interest-bearing obligations, investment-grade instruments or guaranteed obligations of the U.S. government.
Purchases of Equity Securities by the Company
We did not purchase any common shares or other equity securities of our company during the fourth quarter ended December 31, 2019.
Recent Sales of Unregistered Equity Securities
On October 1, 2019, we issued a warrant to purchase up to 50,000 common shares at an exercise price equal to $4.00 per share to Craig-Hallum Capital Group LLC in consideration for certain strategic advisory services. The warrant is exercisable for a term of five years. The warrant includes a cashless exercise provision entitling Craig-Hallum to surrender a portion of the underlying common shares that has a value equal to the aggregate exercise price in lieu of paying cash upon exercise. The warrant was issued to Craig-Hallum in reliance on the exemption from registration provided by Section 4(a)(2) of the Securities Act since the issuance did not involve a public offering, the recipient took the securities for investment and not resale, and we took appropriate measures to restrict transfer.
We did not sell any other unregistered equity securities of our company during the fourth quarter ended December 31, 2019.
Exchange Controls
There are no governmental laws, decrees or regulations in Canada that restrict the export or import of capital, including foreign exchange controls, or that affect the remittance of dividends, interest or other payments to non-resident holders of the securities of DiaMedica, other than Canadian withholding tax.
Certain Canadian Federal Income Tax Considerations for U.S. Holders
The following is, as of March 10, 2020, a summary of the principal Canadian federal income tax considerations under the Income Tax Act (Canada) (Tax Act) generally applicable to a holder of our common shares who, for purposes of the Tax Act and at all relevant times, is neither resident in Canada nor deemed to be resident in Canada for purposes of the Tax Act and any applicable income tax treaty or convention, and who does not use or hold (and is not deemed to use or hold) common shares in the course of carrying on a business in Canada, deals at arm’s length with us, is not affiliated with us, is not a “specified shareholder” of us (within the meaning of subsection 18(5) of the Tax Act) and holds our common shares as capital property (Holder). A “specified shareholder” for these purposes generally includes a person who (either alone or together with persons with whom that person is not dealing at arm’s length for the purposes of the Tax Act) owns or has the right to acquire or control 25% or more of the common shares determined on a votes or fair market value basis. Generally, common shares will be considered to be capital property to a Holder thereof provided that the Holder does not hold common shares in the course of carrying on a business and such Holder has not acquired them in one or more transactions considered to be an adventure or concern in the nature of trade.
This summary does not apply to a Holder, (i) that is a “financial institution” for purposes of the mark-to-market rules contained in the Tax Act; (ii) that is a “specified financial institution” as defined in the Tax Act; (iii) that holds an interest which is a “tax shelter investment” as defined in the Tax Act; or (iv) that has elected to report its tax results in a functional currency other than Canadian currency. Special rules, which are not discussed in this summary, may apply to a Holder that is an “authorized foreign bank” within the meaning of the Tax Act, a partnership or an insurer carrying on business in Canada and elsewhere. Such Holders should consult their own tax advisors.
This summary is based upon the provisions of the Tax Act (including the regulations (Regulations) thereunder) in force as of March 10, 2020 and our understanding of the current administrative policies and assessing practices of the Canada Revenue Agency (CRA) published in writing by the CRA prior to March 10, 2020. This summary takes into account all specific proposals to amend the Tax Act (and the Regulations) publicly announced by or on behalf of the Minister of Finance (Canada) prior to the date hereof (Tax Proposals) and assumes that the Tax Proposals will be enacted in the form proposed, although no assurance can be given that the Tax Proposals will be enacted in their current form or at all. This summary does not otherwise take into account any changes in law or in the administrative policies or assessing practices of the CRA, whether by legislative, governmental or judicial decision or action. This summary is not exhaustive of all possible Canadian federal income tax considerations and does not take into account other federal or any provincial, territorial or foreign income tax legislation or considerations, which may differ materially from those described in this summary.
This summary is of a general nature only and is not, and is not intended to be, and should not be construed to be, legal or tax advice to any particular Holder, and no representations concerning the tax consequences to any particular Holder are made. Holders should consult their own tax advisors regarding the income tax considerations applicable to them having regard to their particular circumstances.
Dividends
Dividends paid or credited (or deemed to be paid or credited) to a Holder by us are subject to Canadian withholding tax at the rate of 25% unless reduced by the terms of an applicable tax treaty or convention. For example, under the Canada-United States Tax Convention (1980), as amended (US Treaty), the dividend withholding tax rate is generally reduced to 15% (or 5% in the case of a Holder that is a company that beneficially owns at least 10% of our voting shares) in respect of a dividend paid or credited to a Holder beneficially entitled to the dividend who is resident in the United States for purposes of the US Treaty and whose entitlement to the benefits of the US Treaty is not limited by the limitation of benefits provisions of the US Treaty. Holders are urged to consult their own tax advisors to determine their entitlement to relief under the US Treaty or any other applicable tax treaty as well as their ability to claim foreign tax credits with respect to any Canadian withholding tax, based on their particular circumstances.
Disposition of Common Shares
A Holder generally will not be subject to tax under the Tax Act in respect of a capital gain realized on the disposition or deemed disposition of a common share, unless the common share constitutes or is deemed to constitute “taxable Canadian property” to the Holder thereof for purposes of the Tax Act, and the gain is not exempt from tax pursuant to the terms of an applicable tax treaty or convention.
In general, provided the common shares are listed on a “designated stock exchange” (which currently includes The Nasdaq Capital Market) at the date of the disposition, the common shares will only constitute “taxable Canadian property” of a Holder if, at any time within the 60-month period preceding the disposition: (i) such Holder, persons with whom the Holder did not deal at arm’s length, partnerships in which the Holder or a person with whom the Holder did not deal at arm’s length holds a membership interest directly or indirectly through one or more partnerships, or any combination thereof, owned 25% or more of the issued shares of any class or series of the Company’s share capital; and (ii) more than 50% of the fair market value of the common shares was derived directly or indirectly from one or any combination of (A) real or immovable property situated in Canada, (B) Canadian resource properties, (C) timber resource properties, and (D) options in respect of, or interests in, or for civil law rights in, property described in any of subparagraphs (ii)(A) to (C), whether or not the property exists. However, and despite the foregoing, in certain circumstances the common shares may be deemed to be “taxable Canadian property” under the Tax Act.
Holders whose common shares may be “taxable Canadian property” should consult their own tax advisers.
Certain U.S. Federal Income Tax Considerations
The following discussion is generally limited to certain material U.S. federal income tax considerations relating to the purchase, ownership and disposition of our common shares by U.S. Holders (as defined below). This discussion applies to U.S. Holders that hold our common shares as capital assets. This summary is for general information purposes only and does not purport to be a complete analysis or listing of all potential U.S. federal income tax considerations that may apply to a U.S. Holder arising from and relating to the acquisition, ownership, and disposition of our common shares. Accordingly, this summary is not intended to be, and should not be construed as, legal or U.S. federal income tax advice with respect to any U.S. Holder. Although this discussion is generally limited to the U.S. federal income tax considerations to U.S. Holders, the U.S. federal income tax treatment of dividends on and gain on sale or exchange of our common shares by certain “Non-U.S. Holders” (as defined below) is included below at “U.S. Federal Income Taxation of Non-U.S. Holders.”
No legal opinion from U.S. legal counsel or ruling from the Internal Revenue Service (IRS) has been requested, or will be obtained, regarding the U.S. federal income tax consequences of the acquisition, ownership, and disposition of common shares. This summary is not binding on the IRS, and the IRS is not precluded from taking a position that is different from, and contrary to, the positions presented in this summary. In addition, because the guidance on which this summary is based are subject to various interpretations, the IRS and the U.S. courts could disagree with one or more of the positions described in this summary.
This discussion is based on the U.S. Internal Revenue Code of 1986, as amended (Code), U.S. Treasury regulations promulgated thereunder and administrative and judicial interpretations thereof, and the income tax treaty between the United States and Canada (Convention), all as in effect on the date hereof and all of which are subject to change, possibly with retroactive effect. This summary is applicable to U.S. Holders who are residents of the United States for purposes of the Convention and who qualify for the full benefits of the Convention. This summary does not discuss the potential effects, whether adverse or beneficial, of any proposed legislation.
This discussion does not address all of the U.S. federal income tax considerations that may be relevant to specific U.S. Holders in light of their particular circumstances or to U.S. Holders subject to special treatment under U.S. federal income tax law (such as certain financial institutions, insurance companies, broker-dealers and traders in securities or other persons that generally mark their securities to market for U.S. federal income tax purposes, tax-exempt entities, retirement plans, regulated investment companies, real estate investment trusts, certain former citizens or residents of the United States, persons who hold common shares as part of a “straddle,” “hedge,” “conversion transaction,” “synthetic security” or integrated investment, persons that have a “functional currency” other than the U.S. dollar, persons that own (or are deemed to own) 10% or more (by voting power or value) of our common shares, persons that acquire their common shares as part of a compensation arrangement, corporations that accumulate earnings to avoid U.S. federal income tax, partnerships and other pass-through entities, and investors in such pass-through entities). This discussion does not address any U.S. state or local or non-U.S. tax considerations or any U.S. federal estate, gift or alternative minimum tax considerations. In addition, except as specifically set forth below, this summary does not discuss applicable tax reporting requirements.
As used in this discussion, the term “U.S. Holder” means a beneficial owner of common shares that is, for U.S. federal income tax purposes, (1) an individual who is a citizen or resident of the United States, (2) a corporation (or entity treated as a corporation for U.S. federal income tax purposes) created or organized in or under the laws of the United States, any state thereof, or the District of Columbia, (3) an estate the income of which is subject to U.S. federal income tax regardless of its source or (4) a trust (x) with respect to which a court within the United States is able to exercise primary supervision over its administration and one or more United States persons have the authority to control all of its substantial decisions or (y) that has elected under applicable U.S. Treasury regulations to be treated as a domestic trust for U.S. federal income tax purposes.
If an entity treated as a partnership for U.S. federal income tax purposes holds the common shares, the U.S. federal income tax considerations relating to an investment in the common shares will depend in part upon the status and activities of such entity and the particular partner. Any such entity should consult its own tax advisor regarding the U.S. federal income tax considerations applicable to it and its partners of the purchase, ownership and disposition of the common shares.
Persons holding common shares should consult their own tax advisors as to the particular tax considerations applicable to them relating to the purchase, ownership and disposition of common shares, including the applicability of U.S. federal, state and local tax laws and non-U.S. tax laws.
Distributions
Subject to the discussion below under “Passive Foreign Investment Company Considerations,” a U.S. Holder that receives a distribution with respect to the common shares generally will be required to include the gross amount of such distribution (before reduction for any Canadian withholding taxes) in gross income as a dividend when actually or constructively received to the extent of the U.S. Holder’s pro rata share of our current and/or accumulated earnings and profits (as determined under U.S. federal income tax principles). To the extent a distribution received by a U.S. Holder is not a dividend because it exceeds the U.S. Holder’s pro rata share of our current and accumulated earnings and profits, it will be treated first as a tax-free return of capital and reduce (but not below zero) the adjusted tax basis of the U.S. Holder’s common shares. To the extent the distribution exceeds the adjusted tax basis of the U.S. Holder’s common shares, the remainder will be taxed as capital gain. However, we cannot provide any assurance that we will maintain or provide earnings and profits determinations in accordance with U.S. federal income tax principles. Therefore, U.S. Holders should expect that a distribution will generally be treated as a dividend even if that distribution would otherwise be treated as a non-taxable return of capital or as capital gain under the rules described above.
The U.S. dollar value of any distribution on the common shares made in Canadian dollars generally should be calculated by reference to the exchange rate between the U.S. dollar and the Canadian dollar in effect on the date of receipt (or deemed receipt) of such distribution by the U.S. Holder regardless of whether the Canadian dollars so received are in fact converted into U.S. dollars at that time. If the Canadian dollars received are converted into U.S. dollars on the date of receipt (or deemed receipt), a U.S. Holder generally should not recognize currency gain or loss on such conversion. If the Canadian dollars received are not converted into U.S. dollars on the date of receipt (or deemed receipt), a U.S. Holder generally will have a basis in such Canadian dollars equal to the U.S. dollar value of such Canadian dollars on the date of receipt (or deemed receipt). Any gain or loss on a subsequent conversion or other disposition of such Canadian dollars by such U.S. Holder generally will be treated as ordinary income or loss and generally will be income or loss from sources within the United States for U.S. foreign tax credit purposes. Different rules apply to U.S. Holders who use the accrual method of tax accounting. Each U.S. Holder should consult its own U.S. tax advisors regarding the U.S. federal income tax consequences of receiving, owning, and disposing of foreign currency.
Distributions on the common shares that are treated as dividends generally will constitute income from sources outside the United States for foreign tax credit purposes and generally will constitute “passive category income.” Because we are not a United States corporation, such dividends will not be eligible for the “dividends received” deduction generally allowed to corporate shareholders with respect to dividends received from U.S. corporations. Dividends paid by a “qualified foreign corporation” to a U.S. Holder who is an individual, trust or estate will generally be treated as “qualified dividend income” and are eligible for taxation at a reduced capital gains rate rather than the marginal tax rates generally applicable to ordinary income provided that a holding period requirement (more than 60 days of ownership, without protection from the risk of loss, during the 121-day period beginning 60 days before the ex-dividend date) and certain other requirements are met. However, if we are a passive foreign investment company (PFIC) for the taxable year in which the dividend is paid or the preceding taxable year (see discussion below under “Passive Foreign Investment Company Considerations”), we will not be treated as a qualified foreign corporation, and therefore the reduced capital gains tax rate described above will not apply. Each U.S. Holder is advised to consult its own tax advisors regarding the availability of the reduced tax rate on dividends.
If a U.S. Holder is subject to Canadian withholding tax on dividends paid on the holder’s common shares (see discussion above under “Material Canadian Federal Income Tax Considerations—Dividends”), the U.S. Holder may be eligible, subject to a number of complex limitations, to claim a credit against its U.S. federal income tax for the Canadian withholding tax imposed on the dividends. However, if U.S. persons collectively own, directly or indirectly, 50% or more of the voting power or value of our common shares it is possible that a portion of any dividends we pay will be considered U.S. source income in proportion to our U.S. source earnings and profits, which could limit the ability of a U.S. Holder to claim a foreign tax credit for the Canadian withholding taxes imposed in respect of such a dividend, although certain elections may be available under the Code and the Convention to mitigate these effects. A U.S. Holder may claim a deduction for the Canadian withholding tax in lieu of a credit, but only for a year in which the U.S. Holder elects to do so for all creditable foreign income taxes. The rules governing the foreign tax credit are complex. Each U.S. Holder is advised to consult its tax advisor regarding the availability of the foreign tax credit under its particular circumstances.
Sale, Exchange or Other Disposition of Common Shares
Subject to the discussion below under “Passive Foreign Investment Company Considerations,” a U.S. Holder generally will recognize capital gain or loss for U.S. federal income tax purposes upon the sale, exchange or other disposition of common shares. The amount of gain recognized will equal the excess of the amount realized (i.e., the amount of cash plus the fair market value of any property received) over the U.S. Holder’s adjusted tax basis in the common shares sold or exchanged. The amount of loss recognized will equal the excess of the U.S. Holder’s adjusted tax basis in the common shares sold or exchanged over the amount realized. Such capital gain or loss generally will be long-term capital gain or loss if, on the date of sale, exchange or other disposition, the common shares were held by the U.S. Holder for more than one year. Net long-term capital gain derived by a non-corporate U.S. Holder with respect to capital assets is currently is subject to tax at reduced rates. The deductibility of a capital loss is subject to limitations. Any gain or loss recognized from the sale, exchange or other disposition of common shares will generally be gain or loss from sources within the United States for U.S. foreign tax credit purposes, except as otherwise provided in an applicable income tax treaty and if an election is properly made under the Code.
Passive Foreign Investment Company Considerations
In general, a corporation organized outside the United States will be treated as a PFIC in any taxable year in which either (1) at least 75% of its gross income is “passive income” or (2) at least 50% of the average quarterly value of its assets is attributable to assets that produce passive income or are held for the production of passive income. Passive income for this purpose generally includes, among other things, dividends, interest, royalties, rents, and gains from commodities transactions and from the sale or exchange of property that gives rise to passive income. Assets that produce or are held for the production of passive income include cash, even if held as working capital or raised in a public offering, marketable securities and other assets that may produce passive income. The average percentage of a corporation’s assets that produce or are held for the production of passive income generally is determined on the basis of the fair market value of the corporation’s assets at the end of each quarter (which may be determined in part by the market value of our common shares, which is subject to change). In determining whether a foreign corporation is a PFIC, a proportionate share of the items of gross income and assets of each corporation in which it owns, directly or indirectly, at least a 25% interest (by value) are taken into account.
Although the tests for determining PFIC status are applied as of the end of each taxable year and are dependent upon a number of factors, some of which are beyond our control, including the value of our assets, the market price of our common shares, and the amount and type of our gross income (i) we believe that we were a PFIC for the taxable year ended December 31, 2016, and (ii) we do not believe that we were a PFIC for the taxable years ended December 31, 2019, 2018 and 2017. Our status as a PFIC is a fact-intensive determination made on an annual basis, and we cannot provide any assurance regarding our PFIC status for the taxable year ending December 31, 2020 or for subsequent taxable years. U.S. Holders who own our common shares for any period during which we are a PFIC will be required to file IRS Form 8621 for each tax year during which they hold our common shares. No opinion of legal counsel or ruling from the IRS concerning our status as a PFIC has been obtained or is currently planned to be requested. However, the determination of our PFIC status is made annually after the close of each taxable year and it is difficult to predict before such determination whether we will be a PFIC for any given taxable year. Even if we determine that we are not a PFIC after the close of a taxable year, there can be no assurance that the IRS will agree with our conclusion. No assurance can be provided regarding our PFIC status, and neither we nor our United States counsel expresses any opinion with respect to our PFIC status.
If we are a PFIC at any time when a non-corporate U.S. Holder owns common shares, and such U.S. Holder does not make a “qualified electing fund” election (“QEF election”) or a “mark-to-market” election, both as described below, such U.S. Holder will generally be subject to federal tax under the excess distribution rules (described below). Under such rules, additional taxes and interest charges would apply to certain distributions by us or to gain upon dispositions of our common shares. If neither of such elections are made, the excess distribution rules apply to (1) distributions paid during a taxable year that are greater than 125% of the average annual distributions paid in the three preceding taxable years, or, if shorter, the U.S. Holder’s holding period for the common shares, and (2) any gain recognized on a sale, exchange or other disposition (which would include a pledge or transfer by gift or death) of common shares. Under the excess distribution rules, the non-corporate U.S. Holder’s tax liability will be determined by allocating such distribution or gain ratably to each day in the U.S. Holder’s holding period for the common shares. The amount allocated to the current taxable year (i.e., the year in which the distribution occurs or the gain is recognized) and any year prior to the first taxable year in which we were a PFIC in the holding period will be taxed as ordinary income earned in the current taxable year and the preferential tax rate applicable to capital gains or dividends received on our common shares would not be available. The amount allocated to other taxable years (i.e., prior years in which we were a PFIC) will be taxed at the highest marginal rate in effect (for individuals or corporations as applicable) for ordinary income in each such taxable year, and an interest charge, generally applicable to the underpayment of tax, will be added to the tax and the preferential tax rate applicable to capital gains or dividends received on our common shares would not be available. These adverse tax consequences would not apply to a pension or profit-sharing trust or other tax-exempt organization that did not borrow funds or otherwise utilize leverage in connection with its acquisition of our common shares. In addition, if a non-electing U.S. Holder who is an individual dies while owning our common shares, such U.S. Holder's successor generally would not receive a step-up in tax basis with respect to such common shares, but instead would have a tax basis equal to the lower of the fair market value of such common shares or the decedent’s tax basis in such common shares.
If we are a PFIC at any time when a U.S. Holder holds our common shares, we will generally continue to be treated as a PFIC with respect to the U.S. Holder for all succeeding years during which the U.S. Holder holds our common shares even if we cease to meet the PFIC gross income test or asset test in a subsequent year. However, if we cease to meet these tests, a U.S. Holder can avoid the continuing impact of the PFIC rules by making a special election (a “Purging Election”) to recognize gain by making a “deemed sale” election with respect to all of the U.S. Holder’s common shares and have such common shares deemed to be sold at their fair market value on the last day of the last taxable year during which we were a PFIC. In addition, for a U.S. Holder making such an election, a new holding period would be deemed to begin for our common shares for purposes of the PFIC rules. After the Purging Election, the common shares with respect to which the Purging Election was made will not be treated as shares in a PFIC unless we subsequently again become a PFIC.
The tax considerations that would apply if we were a PFIC would be different from those described above if a U.S. Holder were able to make a valid QEF election. For each year that we meet the PFIC gross income test or asset test, an electing U.S. Holder would be required to include in gross income its pro rata share of our ordinary income and net capital gains, if any, as determined under U.S. federal income tax principles. The U.S. Holder’s adjusted tax basis in our common shares would be increased by the amount of such inclusions. An actual distribution to the U.S. Holder out of such income generally would not be treated as a dividend and would decrease the U.S. Holder’s adjusted tax basis in our common shares. Gain realized from the sale of our common shares covered by a QEF election would be taxed as a capital gain and the denial of the basis step-up at death described above would not apply. Generally, a QEF election must be made by the U.S. Holder in a timely filed tax return for the first taxable year in which the U.S. Holder held our common shares that includes the close of our taxable year for which we met the PFIC gross income test or asset test. A separate QEF election would need to be made for any of our subsidiaries that are classified as a PFIC. A QEF election is made on IRS Form 8621. U.S. Holders will be eligible to make QEF elections only if we agree to provide U.S. Holders with the information they will need to comply with the QEF rules. In the event we become a PFIC, we intend to provide all information and documentation that a U.S. Holder making a QEF election is required to obtain for U.S. federal income tax purposes (e.g., the U.S. Holder’s pro rata share of ordinary income and net capital gain, and a “PFIC Annual Information Statement” as described in applicable U.S. Treasury regulations).
As an alternative to a QEF election, a U.S. Holder may also mitigate the adverse tax consequences of PFIC status by timely making a “mark-to-market” election, provided the U.S. Holder completes and files IRS Form 8621 in accordance with the relevant instructions and related Treasury regulations. A U.S. Holder who makes the mark-to-market election generally must include as ordinary income each year the increase in the fair market value of the common shares and deduct from gross income the decrease in the value of such shares during each of its taxable years, but with losses limited to the amount of previously recognized net gains. The U.S. Holder’s tax basis in the common shares would be adjusted to reflect any income or loss recognized as a result of the mark-to-market election. If a mark-to-market election with respect to our common shares is in effect on the date of a U.S. Holder’s death, the tax basis of the common shares in the hands of a U.S. Holder who acquired them from a decedent will be the lesser of the decedent’s tax basis or the fair market value of the common shares. Any gain from a sale, exchange or other disposition of the common shares in any taxable year in which we are a PFIC (i.e., when we meet the gross income test or asset test described above) would be treated as ordinary income and any loss from a sale, exchange or other disposition would be treated first as an ordinary loss (to the extent of any net mark-to-market gains previously included in income) and thereafter as a capital loss. If we cease to be a PFIC, any gain or loss recognized by a U.S. Holder on the sale or exchange of the common shares would be classified as a capital gain or loss.
A mark-to-market election is available to a U.S. Holder only for “marketable stock.” Generally, stock will be considered marketable stock if it is “regularly traded” on a “qualified exchange” within the meaning of applicable U.S. Treasury regulations. A class of stock is regularly traded during any calendar year during which such class of stock is traded, other than in de minimis quantities, on at least 15 days during each calendar quarter. The common shares should be marketable stock as long as they are listed on The Nasdaq Capital Market and are regularly traded. A mark-to-market election will not apply to the common shares for any taxable year during which we are not a PFIC but will remain in effect with respect to any subsequent taxable year in which we again become a PFIC. Such election will not apply to any subsidiary that we own. Accordingly, a U.S. Holder may continue to be subject to the PFIC rules with respect to any lower-tier PFICs notwithstanding the U.S. Holder’s mark-to-market election. Whether our common shares are regularly traded on a qualified exchange is an annual determination based on facts that, in part, are beyond our control. Accordingly, a U.S. Holder might not be eligible to make a mark-to-market election to mitigate the adverse tax consequences if we are characterized as a PFIC.
Each U.S. person who is a shareholder of a PFIC generally must file an annual report (on IRS Form 8621) with the IRS containing certain information, and the failure to file such report could result in the imposition of penalties on such U.S. person and in the extension of the statute of limitations with respect to federal income tax returns filed by such U.S. person.
The U.S. federal income tax rules relating to PFICs are very complex. U.S. Holders are urged to consult their own tax advisors with respect to the purchase, ownership and disposition of common shares, the consequences to them of an investment in a PFIC, any elections available with respect to the common shares and the IRS information reporting obligations with respect to the purchase, ownership and disposition of common shares in the event we are considered a PFIC.
Additional Tax on Passive Income
Certain U.S. Holders that are individuals, estates or trusts (other than trusts that are exempt from tax) with adjusted income exceeding certain thresholds, will be subject to a 3.8% tax on all or a portion of their “net investment income,” which includes dividends on the common shares, and net gains from the disposition of the common shares. Further, excess distributions treated as dividends, gains treated as excess distributions, and mark-to-market inclusions and deductions are all included in the calculation of net investment income.
Treasury regulations provide, subject to the election described in the following paragraph, that solely for purposes of this additional tax, that distributions of previously taxed income will be treated as dividends and included in net investment income subject to the additional 3.8% tax. Additionally, to determine the amount of any capital gain from the sale or other taxable disposition of common shares that will be subject to the additional tax on net investment income, a U.S. Holder who has made a QEF election will be required to recalculate its basis in the common shares excluding any QEF election basis adjustments.
Alternatively, a U.S. Holder may make an election which will be effective with respect to all interests in controlled foreign corporations and PFICs that are subject to a QEF election and that are held in that year or acquired in future years. Under this election, a U.S. Holder pays the additional 3.8% tax on QEF election income inclusions and on gains calculated after giving effect to related tax basis adjustments. U.S. Holders that are individuals, estates or trusts should consult their own tax advisors regarding the applicability of this tax to any of their income or gains in respect of the common shares.
U.S. Federal Income Taxation of Non-U.S. Holders
A beneficial owner of our common shares, other than a partnership or entity treated as a partnership for U.S. Federal income tax purposes, that is not a U.S. Holder is referred to herein as a “Non-U.S. Holder”. Non-U.S. Holders generally will not be subject to U.S. federal income tax or withholding tax on dividends received from us with respect to our common shares, unless that income is effectively connected with the Non-U.S. Holder’s conduct of a trade or business in the United States. In general, if the Non-U.S. Holder is entitled to the benefits of certain U.S. income tax treaties with respect to those dividends, that income is taxable only if it is attributable to a permanent establishment maintained by the Non-U.S. Holder in the United States.
Non-U.S. Holders generally will not be subject to U.S. federal income tax or withholding tax on any gain realized upon the sale, exchange or other disposition of our common shares, unless:
|
● |
the gain is effectively connected with the Non-U.S. Holder’s conduct of a trade or business in the United States. In general, if the Non-U.S. Holder is entitled to the benefits of certain income tax treaties with respect to that gain, that gain is taxable only if it is attributable to a permanent establishment maintained by the Non-U.S. Holder in the United States; or |
|
● |
the Non-U.S. Holder is an individual who is present in the United States for 183 days or more during the taxable year of disposition and other conditions are met. |
If the Non-U.S. Holder is engaged in a U.S. trade or business for U.S. federal income tax purposes, the income from the common shares, including dividends and the gain from the sale, exchange or other disposition of the stock, that is effectively connected with the conduct of that trade or business will generally be subject to regular U.S. federal income tax in the same manner as discussed above relating to the general taxation of U.S. Holders. In addition, if you are a corporate Non-U.S. Holder, your earnings and profits that are attributable to the effectively connected income, which are subject to certain adjustments, may be subject to an additional branch profits tax at a rate of 30%, or at a lower rate as may be specified by an applicable U.S. income tax treaty.
Information Reporting with Respect to Foreign Financial Assets
U.S. individuals that own “specified foreign financial assets” (as defined in Section 6038D of the Code) with an aggregate fair market value exceeding certain threshold amounts generally are required to file an information report on IRS Form 8938 with respect to such assets with their tax returns. Significant penalties may apply to persons who fail to comply with these rules. Specified foreign financial assets include not only financial accounts maintained in foreign financial institutions, but also, unless held in accounts maintained by certain financial institutions, any stock or security issued by a non-U.S. person, such as our common shares. Upon the issuance of future U.S. Treasury regulations, these information reporting requirements may apply to certain U.S. entities that own specified foreign financial assets. The failure to report information required under the current regulations could result in substantial penalties and in the extension of the statute of limitations with respect to federal income tax returns filed by a U.S. Holder. U.S. Holders should consult their own tax advisors regarding the possible implications of these U.S. Treasury regulations for an investment in our common shares.
Special Reporting Requirements for Transfers to Foreign Corporations
A U.S. Holder that acquires common shares generally will be required to file IRS Form 926 with the IRS if (1) immediately after the acquisition such U.S. Holder, directly or indirectly, owns at least 10% of our common shares, or (2) the amount of cash transferred in exchange for common shares during the 12-month period ending on the date of the acquisition exceeds USD $100,000. Significant penalties may apply for failing to satisfy these filing requirements. U.S. Holders are urged to contact their tax advisors regarding these filing requirements.
Information Reporting and Backup Withholding
Dividends on and proceeds from the sale or other disposition of common shares may be reported to the IRS unless the U.S. Holder establishes a basis for exemption. Backup withholding may apply to amounts subject to reporting if (1) the U.S. holder fails to provide an accurate taxpayer identification number or otherwise establish a basis for exemption, (2) the U.S. Holder is notified by the IRS that backup withholding applies, or (3) the payment is described in certain other categories of persons.
If you sell your common shares through a U.S. office of a broker, the payment of the proceeds is subject to both U.S. backup withholding and information reporting unless you certify that you are a non-U.S. person, under penalties of perjury, or you otherwise establish an exemption. If you sell your common shares through a non-U.S. office of a non-U.S. broker and the sales proceeds are paid to you outside the United States, then information reporting and backup withholding generally will not apply to that payment. However, U.S. information reporting requirements, but not backup withholding, will apply to a payment of sales proceeds, even if that payment is made to you outside the United States, if you sell your common shares through a non-U.S. office of a broker that is a U.S. person or has certain other contacts with the United States, unless you certify that you are a non-U.S. person, under penalty of perjury, or you otherwise establish an exemption.
Backup withholding is not an additional tax. Any amounts withheld under the backup withholding rules generally will be allowed as a refund or a credit against a U.S. Holder’s U.S. federal income tax liability if the required information is furnished by the U.S. Holder on a timely basis to the IRS.
THE DISCUSSION ABOVE IS A GENERAL SUMMARY. IT DOES NOT COVER ALL TAX MATTERS THAT MAY BE OF IMPORTANCE TO A U.S. HOLDER. EACH U.S. HOLDER IS URGED TO CONSULT ITS OWN TAX ADVISOR ABOUT THE TAX CONSEQUENCES TO IT OF AN INVESTMENT IN COMMON SHARES IN LIGHT OF THE INVESTOR’S OWN CIRCUMSTANCES.
|
Item 6. |
Selected Financial Data |
The following tables present, as of the dates and for the periods indicated, our selected historical financial data as indicated therein. The consolidated statements of operations data for the years ended December 31, 2019 and 2018 and the consolidated balance sheet data as of December 31, 2019 and 2018 are derived from our audited financial statements that are included elsewhere in this annual report on Form 10-K. Our historical results are not indicative of the results to be expected in the future.
This information should be read together with our consolidated financial statements and the related notes, as well as the section entitled “Management’s Discussion and Analysis of Financial Condition and Results of Operations” included elsewhere in this report.
|
Year Ended December 31, |
||||||||
|
2019 |
2018 |
|||||||
|
(in thousands, except share and per share data) |
||||||||
|
Consolidated Statements of Operations Data: |
||||||||
|
Operating revenues: |
||||||||
|
License revenue |
$ | — | $ | 500 | ||||
|
Operating expenses: |
||||||||
|
Research and development |
7,900 | 4,522 | ||||||
|
General and administrative |
3,693 | 2,739 | ||||||
|
Total operating expenses |
11,593 | 7,261 | ||||||
|
Loss from operations |
(11,593 | ) | (6,761 | ) | ||||
|
Other (income) expense |
||||||||
|
Governmental assistance – research incentives |
(856 | ) | (1,214 | ) | ||||
|
Other (income) expense |
(119 | ) | 68 | |||||
|
Change in fair value of warrant liability |
— | 39 | ||||||
|
Total other (income) expense |
(975 | ) | (1,107 | ) | ||||
|
Loss before income tax and other comprehensive income |
(10,618 | ) | (5,654 | ) | ||||
|
Income tax |
31 | 80 | ||||||
|
Unrealized gain on marketable securities |
(2 | ) | — | |||||
|
Net loss and comprehensive loss |
$ | (10,647 | ) | $ | (5,734 | ) | ||
|
Loss per share, basic and diluted |
$ | (0.89 | ) | $ | (0.74 | ) | ||
|
Weighted average number of shares outstanding: |
||||||||
|
Basic and diluted |
11,987,696 | 7,743,520 | ||||||
|
December 31, |
||||||||
|
2019 |
2018 |
|||||||
|
Consolidated Balance Sheet: |
||||||||
|
Cash and short-term investments |
$ | 7,878 | $ | 16,823 | ||||
|
Working capital |
7,518 | 16,676 | ||||||
|
Total assets |
9,053 | 18,339 | ||||||
|
Total current liabilities |
1,317 | 1,296 | ||||||
|
Total shareholders’ equity |
7,617 | 17,025 | ||||||
|
Item 7. |
Management’s Discussion and Analysis of Financial Condition and Results of Operations |
The following Management’s Discussion and Analysis of Financial Condition and Results of Operations is based upon accounting principles generally accepted in the United States of America and discusses the financial condition and results of operations for DiaMedica Therapeutics Inc. and subsidiaries for the years ended December 31, 2019 and 2018.
This discussion should be read in conjunction with our consolidated financial statements and related notes included elsewhere in this report. The following discussion contains forward-looking statements that involve numerous risks and uncertainties. Our actual results could differ materially from the forward-looking statements as a result of these risks and uncertainties. See “Cautionary Note Regarding Forward-Looking Statements” for additional cautionary information.
Business Overview
We are a clinical stage biopharmaceutical company primarily focused on the development of novel recombinant proteins. Our goal is to use our patented and licensed technologies and trade secrets to establish our company as a leader in the development and commercialization of therapeutic treatments for novel recombinant proteins. Our current focus is on CKD and AIS. We plan to advance DM199, our lead drug candidate, through required clinical trials to create shareholder value by establishing its clinical and commercial potential as a therapy for CKD and AIS.
DM199 is a recombinant form of human tissue kallikrein-1 (KLK1). KLK1 is a serine protease (protein) produced primarily in the kidneys, pancreas and salivary glands, which plays a critical role in the regulation of local blood flow and vasodilation (the widening of blood vessels which decreases vascular resistance) in the body, as well as an important role in inflammation and oxidative stress (an imbalance between potentially damaging reactive oxygen species, or free radicals, and antioxidants in your body). We believe DM199 has the potential to treat a variety of diseases where healthy functioning requires sufficient activity of KLK1 and its system, the kallikrein-kinin system (KKS).
Our DM199 product candidate is in clinical development as follows:
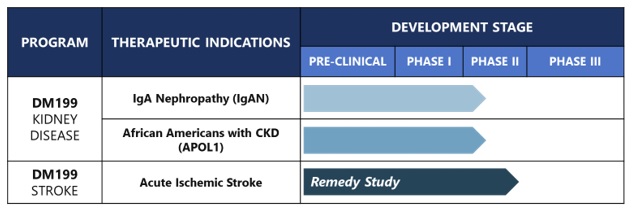
During 2019, DiaMedica initiated and completed a Phase Ib clinical trial of DM199 in 32 subjects with moderate or severe CKD caused by Type I or Type II diabetes mellitus. The study was performed at 3 sites in the U.S. and was designed to assess the pharmacokinetics (PK) of three dose levels of DM199 (3, 5 and 8 µg/kg), administered in a single subcutaneous (SC) dose, as well as the evaluation of safety, tolerability and secondary pharmacodynamic (PD) endpoints. Results from the study were also used to guide the design of Phase II CKD studies.
In October 2019, the FDA accepted our Phase II clinical trial protocol for the treatment of CKD caused by rare or significant unmet diseases. The trial named REDUX, Latin for restore, is a multi-center, open-label investigation of approximately 60 participants with CKD, who are being enrolled in two cohorts (30 participants per cohort). The study is being conducted in the United States at up to 12 sites and is focused on participants with CKD: Cohort I is focused on non-diabetic, hypertensive African Americans with Stage II or III CKD. African Americans are at greater risk for CKD than Caucasians, and those who have the APOL1 gene mutation are at an even higher risk. The study is designed to capture the APOL1 gene mutation as an exploratory biomarker in this cohort; Cohort II is focused on participants with IgA Nephropathy (IgAN). The study will evaluate two dose levels of DM199 within each cohort. Study participants will receive DM199 by subcutaneous injection twice weekly for 95 days. The primary study endpoints include safety, tolerability, blood pressure, albuminuria and kidney function, which will be evaluated by changes from baseline in eGFR and albuminuria, as measured by the UACR. Participant enrollment and dosing for this study commenced in December 2019.
We are currently experiencing slower than expected enrollment in the REDUX clinical trial. In addition, the novel strain of coronavirus (COVID: 19) has adversely affected and may continue to adversely affect our ability to recruit or enroll subjects. If this slow enrollment continues, the completion of these studies will take longer than expected.
In February 2018, treatment was initiated for the first patient in our Phase II REMEDY trial assessing the safety, tolerability and markers of therapeutic efficacy of DM199 in patients suffering from AIS. Our REMEDY trial was expected to enroll up to 100 patients to evaluate DM199 in patients with AIS. The study drug (DM199 or placebo) will be administered as an intravenous (IV) infusion within 24 hours of stroke symptom onset, followed by SC injections later that day and once every 3 days for 21 days. The study was designed to measure safety and tolerability along with multiple tests designed to investigate DM199’s therapeutic potential including plasma-based biomarkers and standard functional stroke measures assessed at 90 days post-stroke. Standard functional stroke measurements include the Modified Rankin Scale, National Institutes of Health Stroke Scale, the Barthel Index and C-reactive protein, a measure of inflammation. In the fourth quarter of 2019, we completed enrollment in the REMEDY trial. Final enrollment was 92 participants.
In September 2018, we entered into a license and collaboration agreement with Ahon Pharma, which granted Ahon Pharma exclusive rights to develop and commercialize DM199 for acute ischemic stroke in mainland China, Taiwan, Hong Kong S.A.R. and Macau S.A.R. Under the terms of the agreement, we received an upfront payment of $500,000 on signing and were entitled to receive an additional payment of $4.5 million upon the earlier of regulatory clearance to initiate a clinical trial in China or July 1, 2019. On August 12, 2019, after extensive good faith discussions with Ahon Pharma, we were unable to agree upon mutually acceptable revised terms to the agreement and we terminated the agreement for non-payment of the $4.5 million milestone, thereby regaining worldwide rights for DM199 for acute ischemic stroke.
On February 13, 2020, we issued and sold an aggregate of 2,125,000 common shares in a public underwritten offering at a public offering price of $4.00 per share, receiving gross proceeds of $8.5 million and net proceeds of approximately $7.7 million, after deducting the underwriting discount and offering expenses. See Note 16 titled “Subsequent Event.”
We have not generated any revenues from product sales. Since our inception, we have financed our operations from public and private sales of equity, the exercise of warrants and stock options, interest income on funds available for investment and government grants and tax credits. We have incurred losses in each year since our inception. Our net losses were $10.6 million and $5.7 million for the years ended December 31, 2019 and 2018, respectively. As of December 31, 2019, we had an accumulated deficit of $56.6 million. Substantially all of our operating losses resulted from expenses incurred in connection with our product candidate development programs, our primary research and development (R&D) activities, and general and administrative (G&A) support costs associated with our operations.
We expect to continue to incur significant expenses and increased operating losses for at least the next several years. In the near term, we anticipate that our expenses will increase as we:
|
● |
advance the ongoing clinical development of DM199; |
|
● |
provide G&A support for our operations; and |
|
● |
maintain, expand and protect our intellectual property portfolio. |
In addition, our operating expenses increased in 2019 compared to 2018 as a result of our Nasdaq-listed U.S. public reporting company status obtained in December 2018.
While we expect our rate of future negative cash flow per month will vary due to the timing of expenses incurred, we expect our current cash resources, together with the $7.7 million in net proceeds from our February 2020 public offering, to be sufficient to allow us to complete our current ongoing Phase II REMEDY trial in patients with AIS and the first two cohorts in the Phase II study in patients with CKD and to otherwise fund our planned operations through 2021. However, the amount and timing of future funding requirements will depend on many factors, including the timing and results of our ongoing development efforts, including enrollment in our clinical trials, the potential expansion of our current development programs, potential new development programs, and related G&A support. We may require significant additional funds earlier than we currently expect and there is no assurance that we will not need or seek additional funding prior to such time. We may elect to raise additional funds even before we need them if market conditions for raising additional capital are favorable.
From a strategic perspective, we continue to believe that strategic alternatives with respect to our DM199 product candidate, including licenses and business collaborations, with other regional and global pharmaceutical and biotechnology companies can be important in advancing the clinical development of DM199. Therefore, as a matter of course and from time to time, we continue to engage in discussions with third parties regarding these matters.
Financial Overview
Revenues
Since our inception, we have incurred losses while advancing the development of our therapeutic product candidates. We have not generated any revenues from product sales and do not expect to do so for a number of years. We may never generate sales revenues from our current DM199 product candidate as we may never succeed in obtaining regulatory approval or commercial sale of this product candidate. We received $500,000 in license revenue during 2018.
Research and Development Expenses
R&D expenses consist primarily of fees paid to external service providers such as contract research organizations and contract manufacturing organizations related to clinical trials, contractual obligations for clinical development, clinical sites, laboratory testing, preclinical trials, development of DM199 and the related manufacturing processes, salaries, benefits, share-based compensation and other personnel costs. We incurred $7.9 million and $4.5 million in R&D expenses for the years ended December 31, 2019 and 2018, respectively. Over the past approximately eight years, our R&D efforts have been primarily focused on developing DM199.
At this time, due to the risks inherent in the clinical development process and the early stage of our product development programs, we are unable to estimate with any certainty the costs we will incur in the continued development of DM199 or any of our preclinical development programs. We expect that our R&D expenses may increase if we are successful in advancing DM199, or any of our preclinical programs, into advanced stages of clinical development. The process of conducting clinical trials necessary to obtain regulatory approval and manufacturing scale-up to support expanded development and potential future commercialization is costly and time consuming. Any failure by us or delay in completing clinical trials, manufacturing scale-up or in obtaining regulatory approvals could lead to increased R&D expenses and, in turn, have a material adverse effect on our results of operations.
General and Administrative Expenses
G&A expenses consist primarily of salaries and related benefits, including share-based compensation related to our executive, finance, business development and support functions. Other G&A expenses include rent and utilities, travel expenses and professional fees for auditing, tax and legal services. We expect that G&A expenses will increase in the future as we expand our operating activities. In 2019, our G&A expenses increased significantly due to increased costs associated with our listing on The Nasdaq Capital Market and U.S. public reporting company status, which commenced in December 2018. This increase in 2019 was partially offset by one-time costs of approximately $360,000 incurred in 2018, associated with the Nasdaq listing process and related legal and accounting fees.
Other (Income) Expense
Other (income) expense consists primarily of governmental assistance comprised of research and development incentives earned by DiaMedica Australia Pty Ltd., interest income and foreign currency exchange gains and losses.
Critical Accounting Policies and Estimates
Management’s discussion and analysis of our financial condition and results of operations is based on our consolidated financial statements, which have been prepared in accordance with U.S. generally accepted accounting principles. The preparation of these consolidated financial statements requires us to make estimates and assumptions for the reported amounts of assets, liabilities, revenue, expenses and related disclosures. Our estimates are based on our historical experience and on various other factors that we believe are reasonable under the circumstances, the results of which form the basis for making judgments about the carrying value of assets and liabilities that are not readily apparent from other sources. Actual results may differ from these estimates under different assumptions or conditions and any such differences may be material.
While our significant accounting policies are more fully described in Note 3 to our consolidated financial statements included elsewhere in this report, we believe the following discussion addresses our most critical accounting policies, which are those that are most important to the portrayal of our financial condition and results of operations and require our most difficult, subjective and complex judgments.
Revenue Recognition
We followed Accounting Standards Codification (ASC) 606, “Revenue from Contracts with Customers” in accounting for our former license and collaboration agreement with Ahon Pharma. Accordingly, the Company recognizes revenue upon transfer of control of the product to our customer in an amount that reflects the consideration we expect to receive in exchange.
We intend to enter into arrangements for the research and development and/or manufacture of products and product candidates. Such arrangements may require us to deliver various rights, services and/or goods, including (i) intellectual property rights or licenses, (ii) R&D services or (iii) manufacturing services. The underlying terms of these arrangements generally would provide for consideration to DiaMedica in the form of nonrefundable, up-front license fees, development and commercial-performance milestone payments, cost sharing, royalty payments and/or profit sharing.
In arrangements involving more than one performance obligation, each required performance obligation is evaluated to determine whether it qualifies as a distinct performance obligation based on whether (i) the customer can benefit from the good or service either on its own or together with other resources that are readily available and (ii) the good or service is separately identifiable from other promises in the contract. The consideration under the arrangement is then allocated to each separate distinct performance obligation based on its respective relative stand-alone selling price. The estimated selling price of each deliverable reflects our best estimate of what the selling price would be if the deliverable was regularly sold by us on a stand-alone basis or using an adjusted market assessment approach if selling price on a stand-alone basis is not available.
The consideration allocated to each distinct performance obligation is recognized as revenue when control of the related goods or services is transferred. Consideration associated with at-risk substantive performance milestones is recognized as revenue when it is probable that a significant reversal of the cumulative revenue recognized will not occur. We intend to utilize the sales and usage-based royalty exception in arrangements that result from the license of intellectual property, recognizing revenues generated from royalties or profit sharing as the underlying sales occur.
Research and Development Costs
Research and development costs include expenses incurred in the conduct of human clinical trials, for third-party service providers performing various treatment, testing and data accumulation and for analysis related to clinical studies; sponsored non-clinical research agreements; developing the manufacturing process necessary to produce sufficient amounts of the DM199 compound for use in our clinical studies; consulting resources with specialized expertise related to execution of our development plan for our DM199 product candidate; and personnel costs, including salaries, benefits and share-based compensation.
We charge research and development costs, including clinical trial costs, to expense when incurred. Our human clinical trials are performed at clinical trial sites and are administered jointly by us with assistance from contract research organizations. Costs of setting up clinical trial sites are accrued upon execution of the study agreement. Expenses related to the performance of clinical trials are accrued based on estimates of work completed to date by CROs, outside contractors and clinical trial sites that manage and perform the trials, and those that manufacture the investigational product. We obtain initial estimates of total costs based on the trial protocol, extent of enrollment of subjects, trial duration, project management costs, manufacturing costs, patient treatment costs and other activities as required by the trial protocol. Additionally, actual costs may be charged to us and are recognized as the tasks are completed by the clinical trial site. Accrued clinical trial costs may be subject to revisions as clinical trials progress and any revisions are recorded in the period in which the facts that give rise to the revisions become known.
Share-based Compensation
We account for all share-based compensation awards using a fair value method. The cost of employee and non-employee services received in exchange for awards of equity instruments is measured and recognized based on the estimated grant date fair value of those awards. Compensation cost is recognized ratably using the straight-line attribution method over the vesting period, which is considered to be the requisite service period. We record forfeitures in the periods in which they occur.
The fair value of share-based awards is estimated using the Black-Scholes option pricing model. The determination of the fair value of share-based awards is affected by our common share price, as well as assumptions regarding a number of complex and subjective variables. Risk-free interest rates are based upon United States Government bond rates appropriate for the expected term of each award. Expected volatility rates are based on the historical volatility equal to the expected life of the option. The assumed dividend yield is zero, as we do not expect to declare any dividends in the foreseeable future. The expected term of options is estimated considering the vesting period at the grant date, the life of the option and the average length of time similar grants have remained outstanding in the past.
The assumptions used in calculating the fair value under the Black-Scholes option valuation model are set forth in the following table for options issued by us for the years ended December 31, 2019 and 2018:
|
2019 |
2018 |
||||||
|
Common share fair value |
$2.07 |
- |
$4.60 | $6.82 |
- |
$7.20 | |
|
Risk-free interest rate |
1.5 | – | 2.4% | 2.1 | – | 2.2% | |
|
Expected dividend yield |
0% | 0% | |||||
|
Expected option life (in years) |
4.2 | – | 5.1 | 4.8 | – | 5.0 | |
|
Expected stock price volatility |
88.7 | – | 103.5% | 123.5 | – | 135.7% | |
Recently Adopted Accounting Pronouncements
In May 2014, the Financial Accounting Standards Board (FASB) issued a new accounting standard that amends the guidance for the recognition of revenue from contracts with customers to transfer goods and services. The FASB subsequently issued additional, clarifying standards to address issues arising from implementation of the new revenue recognition standard. The new revenue recognition standard and clarifying standards require an entity to recognize revenue when control of promised goods or services is transferred to the customer at an amount that reflects the consideration to which the entity expects to be entitled in exchange for those goods or services. We adopted this new standard as of January 1, 2018, but the adoption as of this date had no impact on our financial statements as we had no revenue until the third quarter of 2018.
In February 2016, the FASB issued Accounting Standards Update (ASU) No. 2016-02, Leases. The guidance in ASU 2016-02 supersedes the lease recognition requirements in the Accounting Standards Codification Topic 840, Leases. ASU 2016-02 requires an entity to recognize assets and liabilities arising from a lease for both financing and operating leases, along with additional qualitative and quantitative disclosures. The new standard requires the immediate recognition of all excess tax benefits and deficiencies in the income statement and requires classification of excess tax benefits as an operating activity as opposed to a financing activity in the statements of cash flows. This standard became effective for us on January 1, 2019.
The FASB has subsequently issued the following amendments to ASU 2016-02, which have the same effective date and transition date of January 1, 2019, and which we collectively refer to as the new leasing standards:
|
● |
ASU No. 2018-01, Leases (Topic 842): Land Easement Practical Expedient for Transition to Topic 842, which permits an entity to elect an optional transition practical expedient to not evaluate under Topic 842 land easements that existed or expired prior to adoption of Topic 842 and that were not previously accounted for as leases under the prior standard, ASC 840, Leases. |
|
● |
ASU No. 2018-10, Codification Improvements to Topic 842, Leases, which amends certain narrow aspects of the guidance issued in ASU 2016-02. |
|
● |
ASU No. 2018-11, Leases (Topic 842): Targeted Improvements, which allows for a transition approach to initially apply ASU 2016-02 at the adoption date and recognize a cumulative-effect adjustment to the opening balance of retained earnings in the period of adoption as well as an additional practical expedient for lessors to not separate non-lease components from the associated lease component. |
|
● |
ASU No. 2018-20, Narrow-Scope Improvements for Lessors, which contains certain narrow scope improvements to the guidance issued in ASU 2016-02. |
We adopted the new leasing standards on January 1, 2019, using a modified retrospective transition approach to be applied to leases existing as of, or entered into after, January 1, 2019; and, consequently, financial information will not be updated and the disclosures required under Topic 842 will not be provided for dates and periods prior to January 1, 2019. We have reviewed our existing lease contracts and the impact of the new leasing standards on our consolidated results of operations, financial position and disclosures. Upon adoption of the new leasing standards, we recognized a lease liability and related right-of-use asset on our consolidated balance sheet of approximately $205,000.
In June 2018, the FASB issued ASU No. 2018-07, “Improvements to Nonemployee Share-Based Payment Accounting,” to simplify the accounting for share-based payments to nonemployees by aligning it with the accounting for share-based payments to employees, with certain exceptions. This ASU is effective for public entities for fiscal years beginning after December 15, 2018. Prior to the adoption of this ASU, share-based compensation awarded to non-employees was subject to revaluation over its vesting terms. Subsequent to the adoption of this ASU, non-employee share-based payment awards are measured on the date of grant, similar to share-based payment awards granted to employees. We adopted this standard on January 1, 2019 and the adoption of this ASU did not have a material impact on our financial position or our consolidated statements of operations.
Results of Operations
Comparison of the Years Ended December 31, 2019 and 2018
The following table summarizes our results of operations for the years ended December 31, 2019 and 2018 (in thousands):
|
Year Ended December 31, |
||||||||
|
2019 |
2018 |
|||||||
|
License revenue |
$ | — | $ | 500 | ||||
|
Research and development |
7,900 | 4,522 | ||||||
|
General and administrative |
3,693 | 2,739 | ||||||
|
Other (income) expense |
(975 | ) | (1,107 | ) | ||||
License Revenue
License revenue for 2018 was comprised of the initial $500,000 license payment we received upon signing of the September 27, 2018 license and collaboration agreement with Ahon Pharma. No license revenue was recognized in 2019.
Research and Development Expenses
R&D expenses were $7.9 million for the year ended December 31, 2019 compared to $4.5 million for the year ended December 31, 2018, an increase of $3.4 million. The increase was due to costs of approximately $1.4 million incurred for a new production run of the DM199 drug substance, as well as costs incurred in conjunction with the Phase Ib and Phase II clinical studies in CKD patients and related non-clinical testing. Increased non-cash share-based compensation costs also contributed to the increase. These increases were partially offset by a reduction in cost incurred in conjunction with the REMEDY Phase II clinical study in AIS patients for which we completed enrollment in October 2019.
General and Administrative Expenses
G&A expenses were $3.7 million and $2.7 million for the years ended December 31, 2019 and 2018, respectively. This $1.0 million increase was primarily due to costs associated with our status as a Nasdaq-listed U.S. public reporting company, which commenced in December 2018, including increased professional service, compliance and non-cash share-based compensation costs. Increased personnel costs also contributed to the increase on a year-to-date basis. This increase was partially offset by one-time costs of approximately $360,000 incurred in 2018, associated with the Nasdaq listing process and related legal and accounting fees.
Other (Income) Expense
Other income, net, was $1.0 million for the year ended December 31, 2019 compared to $1.1 million for 2018. This decrease is primarily related to the initial recognition of R&D incentives, from the Australian Government, paid for qualifying research work performed by DiaMedica Australia Pty Ltd. during 2018, which included research work performed in 2017 and 2018. The decrease was partially offset by increased interest income earned on marketable securities during 2019.
Liquidity and Capital Resources
The following table summarizes our liquidity and capital resources as of December 31, 2019 and 2018 and for each of the years ended December 31, 2019 and 2018, and is intended to supplement the more detailed discussion that follows (in thousands):
|
Liquidity and Capital Resources |
2019 |
2018 |
||||||
|
Cash, cash equivalents and marketable securities |
$ | 7,878 | $ | 16,823 | ||||
|
Total assets |
9,053 | 18,339 | ||||||
|
Total current liabilities |
1,318 | 1,296 | ||||||
|
Total shareholders’ equity |
7,617 | 17,025 | ||||||
|
Working capital |
7,518 | 16,676 | ||||||
|
Year Ended December 31, |
||||||||
|
Cash Flow Data |
2019 |
2018 |
||||||
|
Cash flow provided by (used in): |
||||||||
|
Operating activities |
$ | (9,102 | ) | $ | (5,696 | ) | ||
|
Investing activities |
(3,908 | ) | (50 | ) | ||||
|
Financing activities |
70 | 21,216 | ||||||
|
Net increase (decrease) in cash |
$ | (12,940 | ) | $ | 15,470 | |||
Working Capital
We had cash, cash equivalents and marketable securities of $7.9 million, current liabilities of $1.3 million and working capital of $7.5 million as of December 31, 2019, compared to $16.8 million in cash and cash equivalents and marketable securities, $1.3 million in current liabilities and $16.7 million in working capital as of December 31, 2018. The decreases in cash, cash equivalents and marketable securities and working capital are mainly due to our use of cash to fund operating activities during 2019.
On February 13, 2020, we issued and sold an aggregate of 2,125,000 common shares in a public underwritten offering at a public offering price of $4.00 per share, receiving gross proceeds of $8.5 million and net proceeds of approximately $7.7 million, after deducting the underwriting discount and offering expenses. See Note 16 titled “Subsequent Event.”
On December 27, 2019, we entered into a litigation funding agreement with LEGALIST FUND II, L.P. (the Funder) for the purpose of funding our currently pending lawsuit against PRA Netherlands. Our management believes, but cannot guarantee, that this litigation funding agreement will allow us to pursue this litigation more effectively. Although the Funder made its evaluation as to the likelihood of success, litigation is very uncertain, and no assurance can be provided that, just because we have obtained litigation funding, we will be successful or that any recovery we may obtain will be significant. Under the terms of the litigation funding agreement, the Funder agreed to pay up to an aggregate of $1.0 million to fund reasonable legal fees, court costs, and other expenses incurred by us in connection with the litigation, including $200,000 for fees and costs previously paid by us. These payments, however, are conditioned upon the transfer of venue of the litigation from Delaware to Minnesota and if the venue is not transferred we will not be entitled to receive any payments under the litigation funding agreement. If the venue is transferred, we agreed to repay the Funder from any proceeds arising from the litigation the amount of costs actually paid or otherwise funded by the Funder in connection with the litigation, plus the reimbursement of $10,000 for its diligence and underwriting costs. Additionally, we agreed to pay the Funder from the Claim Proceeds the greater of: (i) $1.0 million if repayment occurs within nine months of the Transfer, $2.0 million if repayment occurs more than nine months after the Transfer but before trial has begun, or $3.0 million thereafter; or (ii) 20% of the Claim Proceeds. In the event the Funder has not been repaid 3½ years after the Transfer, the Funder is entitled to receive interest on the unpaid amounts equal to 20% per annum commencing on the 3½ year anniversary of the Transfer. Our obligation under the litigation funding agreement to make the foregoing payments to the Funder is non-recourse and limited only to the Claim Proceeds. As a result of the agreement, if we obtain Claim Proceeds, it is possible, depending on the amount of the Claim Proceeds, that we will receive no net recovery after all payments have been made to the Funder.
Cash Flows
Operating Activities
Net cash used in operating activities for the year ended December 31, 2019 was $9.1 million compared to $5.7 million for the year ended December 31, 2018. This increase relates primarily to an increase in the net loss, partially offset by non-cash expenses and the effects of the changes in operating assets and liabilities.
Investing Activities
Investing activities consist primarily of purchases of marketable securities and property and equipment. Net cash used in investing activities was $3.9 million for the year ended December 31, 2019 compared to $50,000 for the year ended December 31, 2018. This increase relates primarily to the investment of excess cash in short-term marketable securities.
Financing Activities
Financing activities consist primarily of net proceeds from the sale of common shares and warrants and proceeds from the exercise of stock options and warrants. Net cash provided by financing activities was $70,000 for the year ended December 31, 2019 compared to $21.2 million for the year ended December 31, 2018. Cash flows from financing activities for 2018 included net proceeds from our December 2018 initial public offering and private placements of our common shares and warrants to purchase common shares in March 2018.
In December 2018, we completed an initial public offering of our common shares in the United States by issuing 4,100,000 common shares at an offering price of $4.00 per share, resulting in net proceeds to us of approximately $14.7 million, after deducting the underwriting discount and offering expenses.
On March 29, 2018, we completed, in two tranches, a brokered and non-brokered private placement of 1,322,965 units at a price of $4.90 per unit for aggregate gross proceeds of approximately $6.3 million. Each unit consisted of one common share and one-half of one common share purchase warrant. Each whole warrant entitles the holder to purchase one common share at a price of $7.00 at any time prior to expiration on March 19, 2020 and March 29, 2020 for tranche 1 and tranche 2, respectively. The warrants are subject to early expiration under certain conditions. In connection with the offering, we paid an aggregate cash fee of approximately $384,000 to brokers and issued an aggregate of 80,510 compensation options. Each compensation option entitles the holder to purchase one common share at $4.90, the offering price, for a period of two years from the closing of the offering, subject to acceleration on the same terms as the warrants issued to the investors.
Capital Requirements
Since our inception, we have incurred losses while advancing the R&D of our product candidates. We have not generated any revenues from product sales and do not expect to do so for a number of years. We do not know when, or if, we will generate any revenues from product sales of our DM199 product candidate or any future product candidates. We do not expect to generate any revenue from product sales unless and until we obtain regulatory approval. We expect to continue to incur substantial operating losses until such time as any future product sales, royalty payments, licensing fees, and/or milestone payments are sufficient to generate revenues to fund our continuing operations. We expect our operating losses to increase in the near term as we continue the research, development and clinical trials of, and seek regulatory approval for, our DM199 product candidate. In addition, our operating expenses increased in 2019 compared to 2018 as a result of our recently obtained Nasdaq-listed U.S. public reporting company status and we expect to continue to incur costs at or above this level. In the long-term, subject to obtaining regulatory approval of our DM199 product candidate or any other future product candidates, we expect to incur significant commercialization expenses for product sales, marketing, manufacturing and distribution.
Accordingly, we expect we will need substantial additional capital to further our R&D activities, planned clinical trials, regulatory activities and otherwise develop our product candidate, DM199, or any future product candidates, to a point where they may be commercially sold. While we are striving to achieve these plans, there is no assurance these and other strategies will be achieved or that additional funding will be obtained on favorable terms or at all. While our rate of future negative cash flow per month will vary due to the timing of expenses incurred, we expect our current cash, cash equivalents and marketable securities, supplemented by the net proceeds of our February 2020 public offering, to be sufficient to allow us to complete our current ongoing Phase II REMEDY trial in patients with AIS and our current Phase Ib trial in patients with CKD and a Phase II study in patients with CKD and to otherwise fund our planned operations through 2021. However, the amount and timing of future funding requirements will depend on many factors, including the timing and results of our ongoing development efforts, the potential expansion of our current development programs, potential new development programs and related G&A support. We may require significant additional funds earlier than we currently expect and there is no assurance that we will not need or seek additional funding prior to such time. We may elect to raise additional funds even before we need them if market conditions for raising additional capital are favorable.
Since our inception, we have financed our operations primarily from public and private sales of equity, the exercise of warrants and stock options, interest income on funds available for investment, and government grants and tax incentives, and we expect to continue this practice for the foreseeable future. We do not have any existing credit facilities under which we could borrow funds. We may seek to raise additional funds through various sources, such as equity and debt financings, or through strategic collaborations and license agreements. We can give no assurances that we will be able to secure additional sources of funds to support our operations, or if such funds are available to us, that such additional financing will be sufficient to meet our needs or on terms acceptable to us. This is particularly true if our clinical data is not positive or economic and market conditions deteriorate.
To the extent we raise additional capital through the sale of equity or convertible debt securities, the ownership interests of our shareholders will be diluted. Debt financing, if available, may involve agreements that include conversion discounts or covenants limiting or restricting our ability to take specific actions, such as incurring additional debt, making capital expenditures or declaring dividends. If we raise additional funds through government or other third-party funding, marketing and distribution arrangements or other collaborations, or strategic alliances or licensing arrangements with third parties, we may have to relinquish valuable rights to our technologies, future revenue streams, research programs or product candidates or grant licenses on terms that may not be favorable to us. The availability of financing will be affected by our clinical data and other results of scientific and clinical research; the ability to attain regulatory approvals; market acceptance of our product candidates; the state of the capital markets generally with particular reference to pharmaceutical, biotechnology, and medical companies; the status of strategic alliance agreements; and other relevant commercial considerations. If adequate funding is not available, we may be required to implement cost reduction strategies; delay, reduce, or eliminate one or more of our product development programs; relinquish significant rights to our technologies, future revenue streams, research programs or product candidates or grant licenses on terms that may not be favorable to us; and/or divest assets or cease operations through a merger, sale, or liquidation of our company.
Commitments and Contingencies
In the normal course of business, we incur obligations to make future payments as we execute our business plan. As of December 31, 2019, we had outstanding commitments, including R&D contracts and other commitments, that are known and committed of approximately $4.9 million over the next 12 months and $0 in the following 12 months. These contracts relate to clinical, and development activities, including the clinical study sites and related professional service providers conducting or supporting the conduct of the REDUX study and the clinical research organization conducting the Phase II clinical trial for DM199 related to AIS. These commitments are subject to significant change and the ultimate amounts due may be materially different as these obligations are affected by, among other factors, the number and pace of patients enrolled, the number of clinical study sites, the amount of time to complete study enrollments and the time required to finalize the analysis and reporting of study results. These commitments are generally cancelable upon 30 days’ notice, with our obligation then limited to costs incurred up to that date. As of December 31, 2019, we had future operating lease commitments totaling approximately $158,000 over the remainder of the lease, of which $66,000 is due over the next 12 months.
We have entered into a license agreement with Catalent Pharma Solutions, LLC whereby we have licensed certain gene expression technology and we contract with Catalent for the manufacture of DM199. Under the terms of this license, certain milestone and royalty payments may become due under this agreement and are dependent upon, among other factors, clinical trials, regulatory approvals and ultimately the successful development of a new drug, the outcome and timing of which is uncertain. As of December 31, 2019, two milestones remain which include $185,000 due upon the initiation of dosing in our first Phase III trial and $185,000 upon our first regulatory approval for commercial sale. Following the launch of our first product, we will also incur a royalty of less than 1% on net sales. The royalty term is indefinite but the license agreement may be canceled by us on 90 days’ prior written notice. The license may not be terminated by Catalent unless we fail to make required milestone and royalty payments.
Off-Balance Sheet Arrangements
During 2019 and 2018, we did not have any off-balance sheet arrangements (as defined by applicable SEC regulations) that are reasonably likely to have a current or future material effect on our financial condition, results of operations, liquidity, capital expenditures or capital resources.
|
Item 7A. |
Quantitative and Qualitative Disclosures About Market Risk |
This Item 7A is inapplicable to DiaMedica as a smaller reporting company and has been omitted pursuant to Item 305(e) of SEC Regulation S-K.
|
Item 8. |
Financial Statements and Supplementary Data |
INDEX TO CONSOLIDATED FINANCIAL STATEMENTS
| Page | |
| Report of Independent Registered Public Accounting Firm | 96 |
| Consolidated Balance Sheets as of December 31, 2019 and 2018 | 97 |
| Consolidated Statements of Operations and Comprehensive Loss for the years ended December 31, 2019 and 2018 | 98 |
| Consolidated Statements of Shareholders’ Equity for the years ended December 31, 2019 and 2018 | 99 |
| Consolidated Statements of Cash Flows for the years ended December 31, 2019 and 2018 | 100 |
| Notes to Consolidated Financial Statements | 101-119 |
REPORT OF INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM
To the Board of Directors and Shareholders of
DiaMedica Therapeutics Inc.
Opinion on the Financial Statements
We have audited the accompanying consolidated balance sheets of DiaMedica Therapeutics Inc. and Subsidiaries (the “Company”) as of December 31, 2019 and 2018, and the related consolidated statements of operations and comprehensive loss, shareholders’ equity (deficit), and cash flows for each of the years then ended, and the related notes (collectively referred to as the “financial statements”). In our opinion, the financial statements present fairly, in all material respects, the financial position of the Company as of December 31, 2019 and 2018, and the results of its operations and its cash flows for each of the years then ended in conformity with accounting principles generally accepted in the United States of America.
Basis for Opinion
These financial statements are the responsibility of the Company’s management. Our responsibility is to express an opinion on the Company’s financial statements based on our audits. We are a public accounting firm registered with the Public Company Accounting Oversight Board of the United States of America (PCAOB) and are required to be independent with respect to the Company in accordance with the U.S. federal securities laws and the applicable rules and regulations of the Securities and Exchange Commission and the PCAOB.
We conducted our audits in accordance with the standards of the PCAOB. Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement, whether due to error or fraud. The Company is not required to have, nor were we engaged to perform, an audit of its internal control over financial reporting. As part of our audits, we are required to obtain an understanding of internal control over financial reporting, but not for the purpose of expressing an opinion on the effectiveness of the Company’s internal control over financial reporting. Accordingly, we express no such opinion.
Our audits included performing procedures to assess the risks of material misstatement of the financial statements, whether due to error or fraud, and performing procedures that respond to those risks. Such procedures included examining, on a test basis, evidence regarding the amounts and disclosures in the financial statements. Our audits also included evaluating the accounting principles used and significant estimates made by management, as well as evaluating the overall presentation of the financial statements. We believe that our audits provide a reasonable basis for our opinion.
/s/ Baker Tilly Virchow Krause, LLP
We have served as the Company’s auditors since 2016.
Minneapolis, MN
March 23, 2020
DiaMedica Therapeutics Inc.
Consolidated Balance Sheets
(In thousands, except share amounts)
|
December 31, 2019 |
December 31, 2018 |
|||||||
|
ASSETS |
||||||||
|
Current assets: |
||||||||
|
Cash and cash equivalents |
$ | 3,883 | $ | 16,823 | ||||
|
Marketable securities |
3,995 | — | ||||||
|
Amounts receivable |
823 | 780 | ||||||
|
Deposits |
88 | — | ||||||
|
Prepaid expenses and other assets |
47 | 369 | ||||||
|
Total current assets |
8,836 | 17,972 | ||||||
|
Non-current assets: |
||||||||
|
Operating lease right-of-use asset |
153 | — | ||||||
|
Property and equipment, net |
64 | 96 | ||||||
|
Deposits |
— | 271 | ||||||
|
Total non-current assets |
217 | 367 | ||||||
|
Total assets |
$ | 9,053 | $ | 18,339 | ||||
|
LIABILITIES AND EQUITY |
||||||||
|
Current liabilities: |
||||||||
|
Accounts payable |
$ | 182 | $ | 483 | ||||
|
Accrued liabilities |
1,076 | 808 | ||||||
|
Finance lease obligation |
6 | 5 | ||||||
|
Operating lease obligation |
54 | — | ||||||
|
Total current liabilities |
1,318 | 1,296 | ||||||
|
Non-current liabilities: |
||||||||
|
Finance lease obligation, non-current |
13 | 18 | ||||||
|
Operating lease obligation, non-current |
105 | — | ||||||
|
Total non-current liabilities |
118 | 18 | ||||||
|
Commitments and contingencies (Note 11) |
||||||||
|
Shareholders’ equity: |
||||||||
|
Common shares, no par value; unlimited authorized; 12,006,874 and 11,956,874 shares issued and outstanding, as of December 31, 2019 and 2018, respectively |
— | — | ||||||
|
Paid-in capital |
64,232 | 62,993 | ||||||
|
Accumulated other comprehensive income |
2 | — | ||||||
|
Accumulated deficit |
(56,617 | ) | (45,968 | ) | ||||
|
Total shareholders’ equity |
7,617 | 17,025 | ||||||
|
Total liabilities and shareholders’ equity |
$ | 9,053 | $ | 18,339 | ||||
See accompanying notes to consolidated financial statements.
DiaMedica Therapeutics Inc.
Consolidated Statements of Operations and Comprehensive Loss
(In thousands, except share and per share amounts)
|
Year Ended December 31, |
||||||||
|
2019 |
2018 |
|||||||
|
Operating revenues: |
||||||||
|
License revenues |
$ | — | $ | 500 | ||||
|
Operating expenses: |
||||||||
|
Research and development |
7,900 | 4,522 | ||||||
|
General and administrative |
3,693 | 2,739 | ||||||
|
Total operating expenses |
11,593 | 7,261 | ||||||
|
Operating loss |
(11,593 | ) | (6,761 | ) | ||||
|
Other (income) expense: |
||||||||
|
Governmental assistance - research incentives |
(856 | ) | (1,214 | ) | ||||
|
Other (income) expense, net |
(119 | ) | 68 | |||||
|
Change in fair value of warrant liability |
— | 39 | ||||||
|
Total other income, net |
(975 | ) | (1,107 | ) | ||||
|
Loss before income tax expense |
(10,618 | ) | (5,654 | ) | ||||
|
Income tax expense |
31 | 80 | ||||||
|
Net loss |
(10,649 | ) | (5,734 | ) | ||||
|
Other comprehensive income |
||||||||
|
Unrealized gain on marketable securities |
(2 | ) | — | |||||
|
Net loss and comprehensive loss |
$ | (10,647 | ) | $ | (5,734 | ) | ||
|
Basic and diluted net loss per share |
$ | (0.89 | ) | $ | (0.74 | ) | ||
|
Weighted average shares outstanding – basic and diluted |
11,987,696 | 7,743,520 | ||||||
See accompanying notes to consolidated financial statements.
DiaMedica Therapeutics Inc.
Consolidated Statements of Shareholders’ Equity
(In thousands, except share amounts)
|
Common Shares |
Paid-In Capital |
Accumulated Other Comprehensive Income |
Accumulated Deficit |
Total Shareholders’ Equity |
||||||||||||||||
|
Balances at December 31, 2017 |
6,370,661 | $ | 41,033 | $ | — | $ | (40,234 | ) | $ | 799 | ||||||||||
|
Issuance of common shares and warrants, net of offering costs of $529 |
1,322,965 | 5,840 | — | — | 5,840 | |||||||||||||||
|
Issuance of common shares, net of offering costs of $1,674 |
4,100,000 | 14,726 | — | — | 14,726 | |||||||||||||||
|
Exercise of common share purchase warrants |
146,294 | 731 | — | — | 731 | |||||||||||||||
|
Exercise of common stock options |
16,954 | 43 | — | — | 43 | |||||||||||||||
|
Share-based compensation expense |
— | 620 | — | — | 620 | |||||||||||||||
|
Net loss |
— | — | — | (5,734 | ) | (5,734 | ) | |||||||||||||
|
Balances at December 31, 2018 |
11,956,874 | $ | 62,993 | $ | — | $ | (45,968 | ) | $ | 17,025 | ||||||||||
|
Exercise of common stock options |
50,000 | 75 | — | — | 75 | |||||||||||||||
|
Share-based compensation expense |
— | 1,164 | — | — | 1,164 | |||||||||||||||
|
Unrealized gain on marketable securities |
— | — | 2 | — | 2 | |||||||||||||||
|
Net loss |
— | — | — | (10,649 | ) | (10,649 | ) | |||||||||||||
|
Balances at December 31, 2019 |
12,006,874 | $ | 64,232 | $ | 2 | $ | (56,617 | ) | $ | 7,617 | ||||||||||
See accompanying notes to consolidated financial statements.
DiaMedica Therapeutics Inc.
Consolidated Statements of Cash Flows
(In thousands, except share amounts)
|
Year Ended December 31, |
||||||||
|
2019 |
2018 |
|||||||
|
Cash flows from operating activities: |
||||||||
|
Net loss |
$ | (10,649 | ) | $ | (5,734 | ) | ||
|
Adjustments to reconcile net loss to net cash used in operating activities: |
||||||||
|
Share-based compensation |
1,164 | 620 | ||||||
|
Amortization of discount on marketable securities |
(74 | ) | — | |||||
|
Non-cash lease expense |
49 | — | ||||||
|
Depreciation |
21 | 15 | ||||||
|
Change in fair value of warrant liability |
— | 39 | ||||||
|
Changes in operating assets and liabilities: |
||||||||
|
Amounts receivable |
(43 | ) | (700 | ) | ||||
|
Prepaid expenses |
322 | (308 | ) | |||||
|
Deposits |
183 | — | ||||||
|
Accounts payable |
(301 | ) | (30 | ) | ||||
|
Accrued liabilities |
226 | 402 | ||||||
|
Net cash used in operating activities |
(9,102 | ) | (5,696 | ) | ||||
|
Cash flows from investing activities: |
||||||||
|
Purchase of marketable securities |
(12,919 | ) | — | |||||
|
Maturities of marketable securities |
9,000 | — | ||||||
|
Disposition of property and equipment, net |
13 | — | ||||||
|
Purchase of property and equipment |
(2 | ) | (50 | ) | ||||
|
Net cash used in investing activities |
(3,908 | ) | (50 | ) | ||||
|
Cash flows from financing activities: |
||||||||
|
Proceeds from exercise of stock options |
75 | 43 | ||||||
|
Principal payments on finance lease obligations |
(5 | ) | — | |||||
|
Proceeds from issuance of common shares, net of offering costs |
— | 14,726 | ||||||
|
Proceeds from issuance of common shares and warrants, net offering costs |
— | 5,840 | ||||||
|
Proceeds from the exercise of common share purchase warrants |
— | 607 | ||||||
|
Net cash provided by financing activities |
70 | 21,216 | ||||||
|
Net increase (decrease) in cash and cash equivalents |
(12,940 | ) | 15,470 | |||||
|
Cash and cash equivalents at beginning of period |
16,823 | 1,353 | ||||||
|
Cash and cash equivalents at end of period |
$ | 3,883 | $ | 16,823 | ||||
|
Supplemental disclosure of cash flow information: |
||||||||
|
Cash paid for income taxes |
$ | 26 | $ | 80 | ||||
|
Cash paid for interest |
$ | 2 | $ | 11 | ||||
|
Supplemental disclosure of non-cash transactions: |
||||||||
|
Reclassification of warrant liability upon warrant exercise |
$ | — | $ | 123 | ||||
|
Assets acquired under capital lease |
$ | — | $ | 24 | ||||
See accompanying notes to consolidated financial statements.
DiaMedica Therapeutics Inc.
Notes to Consolidated Financial Statements
|
1. |
Business |
DiaMedica Therapeutics Inc. and its wholly-owned subsidiaries, DiaMedica USA, Inc. and DiaMedica Australia Pty Ltd. (collectively “we,” “us,” “our,” “DiaMedica” and the “Company”), exist for the primary purpose of advancing the clinical and commercial development of a proprietary recombinant KLK1 protein for the treatment of kidney and neurological diseases. Currently, our primary focus is on chronic kidney disease (CKD) and acute ischemic stroke (AIS). Our parent company is governed under the British Columbia Business Corporations Act and, commencing on December 7, 2018, our common shares are publicly traded on The Nasdaq Capital Market under the symbol “DMAC.” The Company’s shares were previously traded on the TSX Venture Exchange in Canada and on the OTCQB in the United States.
Effective November 15, 2018, we implemented a 1-for-20 consolidation of our common shares. No fractional shares were issued in connection with the share consolidation. Instead, the Company rounded to the nearest whole number the number of shares shareholders were entitled to receive in connection with the consolidation. The share consolidation was approved by our shareholders as of November 6, 2018 and was implemented to increase the market price per common share to a level that qualified for listing on The Nasdaq Capital Market. Proportional adjustments were also made to common shares reserved for issuance under the Company’s equity-based compensation plans and outstanding stock options, deferred share units and warrants. All references to share and per share amounts included in these consolidated financial statements have been retroactively restated to reflect the share consolidation.
|
2. |
Risks and Uncertainties |
DiaMedica operates in a highly regulated and competitive environment. The development, manufacturing and marketing of pharmaceutical products require approval from, and are subject to ongoing oversight by, the Food and Drug Administration (FDA) in the United States, the European Medicines Agency (EMA) in the European Union and comparable agencies in other countries. We are in the clinical stage of development of our initial product candidate, DM199, for the treatment of CKD and AIS. The Company has not completed the development of any product candidate and, accordingly, has not begun to commercialize any product candidate or generate any revenues from the commercial sale of any product candidate. DM199 requires significant additional clinical testing and investment prior to seeking marketing approval and is not expected to be commercially available for at least three to five years, if at all. The Company’s future success is dependent upon the success of its development efforts, its ability to demonstrate clinical progress for its DM199 product candidate in the United States or other markets, its ability to obtain required governmental approvals of its product candidate, its ability to license or market and sell its DM199 product candidate and its ability to obtain additional financing to fund these efforts.
As of December 31, 2019, we have incurred losses of $56.6 million since our inception in 2000. For the year ended December 31, 2019, we incurred a net loss of $10.6 million and negative cash flows from operating activities of $9.1 million. We expect to continue to incur operating losses until such time as any future product sales, royalty payments, licensing fees and/or milestone payments are sufficient to generate revenue to fund our continuing operations. Further, we expect our operating losses to continue as we pursue the research, development and clinical trials of, and to seek regulatory approval for, our product candidate. In addition, we expect our operating expenses to increase in 2020 compared to 2019 to support our ongoing clinical and organizational development. As of December 31, 2019, we had cash, cash equivalents and short-term investments of $7.9 million, working capital of $7.5 million and shareholders’ equity of $7.6 million. On February 13, 2020, we issued and sold an aggregate of 2,125,000 common shares in a public underwritten offering at a public offering price of $4.00 per share, receiving gross proceeds of $8.5 million and net proceeds of approximately $7.7 million, after deducting the underwriting discount and offering expenses. See Note 17 titled “Subsequent Event.”
Our principal sources of cash have included net proceeds from the issuance of equity securities. See Note 12 titled “Shareholders’ Equity” and Note 17 titled “Subsequent Event” for additional information. Although the Company has previously been successful in obtaining financing through equity securities offerings, there is no assurance that we will be able to do so in the future. This is particularly true if our clinical data is not positive or economic and market conditions deteriorate.
We expect that we will need substantial additional capital to further our research and development activities, complete the required clinical trials, regulatory activities and otherwise develop our product candidate, DM199, or any future product candidates, to a point where they may be commercially sold. We expect our current cash, supplemented by the net proceeds of our February 2020 public offering, to be sufficient to allow us to complete our currently ongoing Phase II REMEDY trial in patients with AIS and currently ongoing Phase II study in patients with CKD and to otherwise fund our planned operations through 2021. However, the amount and timing of our future funding requirements will depend on many factors, including the timing and results of ongoing development efforts, the potential expansion of current development programs, potential new development programs and related general and administrative support. We may require significant additional funds earlier than we currently expect and there is no assurance that we will not need or seek additional funding prior to such time.
|
3. |
Summary of Significant Accounting Policies |
Basis of consolidation
The accompanying consolidated financial statements include the assets, liabilities and expenses of DiaMedica Therapeutics Inc., and our wholly-owned subsidiaries, DiaMedica USA, Inc. and DiaMedica Australia Pty Ltd. All significant intercompany transactions and balances have been eliminated in consolidation.
Functional currency
The United States dollar is our functional currency as it represents the economic effects of the underlying transactions, events and conditions and various other factors including the currency of historical and future expenditures and the currency in which funds from financing activities are mostly generated by the Company. A change in the functional currency occurs only when there is a material change in the underlying transactions, events and condition. A change in functional currency could result in material differences in the amounts recorded in the consolidated statement of loss and comprehensive loss for foreign exchange gains and losses. All amounts in the accompanying consolidated financial statements are in U.S. dollars unless otherwise indicated.
Use of estimates
The preparation of consolidated financial statements in conformity with accounting principles generally accepted in the United States of America requires management to make estimates and assumptions that affect the amounts reported in the financial statements and the accompanying notes. Actual results could differ from those estimates.
Cash and cash equivalents
The Company considers all bank deposits, including money market funds, and other investments, purchased with an original maturity to the Company of three months or less, to be cash and cash equivalents. The carrying amount of our cash equivalents approximates fair value due to the short maturity of the investments.
Concentration of credit risk
Financial instruments that potentially expose the Company to concentration of credit risk consist primarily of cash, cash equivalents and marketable securities. The Company maintains its cash balances primarily with two financial institutions. These balances generally exceed federally insured limits. The Company has not experienced any losses in such accounts and believes it is not exposed to any significant credit risk in cash and cash equivalents. The Company believes that the credit risk related to marketable securities is limited due to the adherence to an investment policy focused on the preservation of principal.
Marketable securities
The Company’s marketable securities typically consist of obligations of the United States government and its agencies and investment grade corporate obligations, which are classified as available-for-sale and included in current assets as they are intended to fund current operations. Securities are valued based on market prices for similar assets using third party certified pricing sources. Available-for-sale securities are carried at fair value with unrealized gains and losses reported as a component of shareholders’ equity in accumulated other comprehensive income (loss). The amortized cost of debt securities is adjusted for amortization of premiums and accretion of discounts to maturity. Such amortization or accretion is included in interest income. Realized gains and losses, if any, are calculated on the specific identification method and are included in other income in the consolidated statements of operations.
Available-for-sale securities are reviewed for possible impairment at least quarterly, or more frequently if circumstances arise that may indicate impairment. When the fair value of the securities declines below the amortized cost basis, impairment is indicated and it must be determined whether it is other than temporary. Impairment is considered to be other than temporary if the Company: (i) intends to sell the security, (ii) will more likely than not be forced to sell the security before recovering its cost, or (iii) does not expect to recover the security’s amortized cost basis. If the decline in fair value is considered other than temporary, the cost basis of the security is adjusted to its fair market value and the realized loss is reported in earnings. Subsequent increases or decreases in fair value are reported as a component of shareholders’ equity in accumulated other comprehensive income (loss). There were no other-than-temporary unrealized losses as of December 31, 2019.
Fair value measurements
Under the authoritative guidance for fair value measurements, fair value is defined as the exit price, or the amount that would be received to sell an asset or paid to transfer a liability in an orderly transaction between market participants as of the measurement date. The authoritative guidance also establishes a hierarchy for inputs used in measuring fair value that maximizes the use of observable inputs and minimizes the use of unobservable inputs by requiring that the most observable inputs be used when available. Observable inputs are inputs market participants would use in valuing the asset or liability developed based on market data obtained from sources independent of the Company. Unobservable inputs are inputs that reflect the Company’s assumptions about the factors market participants would use in valuing the asset or liability developed based upon the best information available in the circumstances. The categorization of financial assets and financial liabilities within the valuation hierarchy is based upon the lowest level of input that is significant to the fair value measurement.
The hierarchy is broken down into three levels defined as follows:
Level 1 Inputs — quoted prices in active markets for identical assets and liabilities
Level 2 Inputs — observable inputs other than quoted prices in active markets for identical assets and liabilities
Level 3 Inputs — unobservable inputs
As of December 31, 2019, the Company believes that the carrying amounts of its other financial instruments, including amounts receivable, accounts payable and accrued liabilities, approximate their fair value due to the short-term maturities of these instruments. See Note 5, titled “Marketable Securities” for additional information.
Long-lived assets
Property and equipment are stated at purchased cost less accumulated depreciation. Depreciation of property and equipment is computed using the straight-line method over their estimated useful lives of three to ten years for office equipment and four years for computer equipment. Upon retirement or sale, the cost and related accumulated depreciation are removed from the consolidated balance sheets and the resulting gain or loss is reflected in the consolidated statements of operations. Repairs and maintenance are expensed as incurred.
Long-lived assets are evaluated for impairment when events or changes in circumstances indicate that the carrying amount of the asset or related group of assets may not be recoverable. If the expected future undiscounted cash flows are less than the carrying amount of the asset, an impairment loss is recognized at that time. Measurement of impairment may be based upon appraisal, market value of similar assets or discounted cash flows.
Revenue recognition
We followed ASC 606, “Revenue from Contracts with Customers” in accounting for our former license and collaboration agreement with Ahon Pharmaceutical Co Ltd. Accordingly, the Company recognizes revenue upon transfer of control of the product to our customer in an amount that reflects the consideration we expect to receive in exchange.
We intend to enter into arrangements for the research and development (R&D) and/or manufacture of products and product candidates. Such arrangements may require us to deliver various rights, services and/or goods, including (i) intellectual property rights or licenses, (ii) R&D services or (iii) manufacturing services. The underlying terms of these arrangements generally would provide for consideration to DiaMedica in the form of nonrefundable, up-front license fees, development and commercial-performance milestone payments, cost sharing, royalty payments and/or profit sharing.
In arrangements involving more than one performance obligation, each required performance obligation is evaluated to determine whether it qualifies as a distinct performance obligation based on whether (i) the customer can benefit from the good or service either on its own or together with other resources that are readily available and (ii) the good or service is separately identifiable from other promises in the contract. The consideration under the arrangement is then allocated to each separate distinct performance obligation based on its respective relative stand-alone selling price. The estimated selling price of each deliverable reflects our best estimate of what the selling price would be if the deliverable was regularly sold by us on a stand-alone basis or using an adjusted market assessment approach if selling price on a stand-alone basis is not available.
The consideration allocated to each distinct performance obligation is recognized as revenue when control of the related goods or services is transferred. Consideration associated with at-risk substantive performance milestones is recognized as revenue when it is probable that a significant reversal of the cumulative revenue recognized will not occur. We intend to utilize the sales and usage-based royalty exception in arrangements that resulted from the license of intellectual property, recognizing revenues generated from royalties or profit sharing as the underlying sales occur.
Research and development costs
Research and development costs include expenses incurred in the conduct of human clinical trials, for third-party service providers performing various treatment, testing and data accumulation and for analysis related to clinical studies; sponsored non-clinical research agreements; developing the manufacturing process necessary to produce sufficient amounts of the DM199 compound for use in our clinical studies; consulting resources with specialized expertise related to execution of our development plan for our DM199 product candidate; and personnel costs, including salaries, benefits and share-based compensation.
We charge research and development costs, including clinical trial costs, to expense when incurred. Our human clinical trials are performed at clinical trial sites and are administered jointly by us with assistance from contract research organizations. Costs of setting up clinical trial sites are accrued upon execution of the study agreement. Expenses related to the performance of clinical trials are accrued based on estimates of work completed to date by CROs, outside contractors and clinical trial sites that manage and perform the trials, and those that manufacture the investigational product. We obtain initial estimates of total costs based on the trial protocol, extent of enrollment of subjects, trial duration, project management costs, manufacturing costs, patient treatment costs and other activities as required by the trial protocol. Additionally, actual costs may be charged to us and are recognized as the tasks are completed by the clinical trial site. Accrued clinical trial costs may be subject to revisions as clinical trials progress and any revisions are recorded in the period in which the facts that give rise to the revisions become known.
Patent costs
Costs associated with applying for, prosecuting and maintaining patents are expensed as incurred given the uncertainty of patent approval and, if approved, the resulting probable future economic benefit to the Company. Patent-related costs, consisting primarily of legal expenses and filing/maintenance fees, are included in research and development costs and were $87,000 and $156,000 for the years ended December 31, 2019 and 2018, respectively.
Share-based compensation
The cost of employee and non-employee services received in exchange for awards of equity instruments is measured and recognized based on the estimated grant date fair value of those awards. Compensation cost is recognized ratably using the straight-line attribution method over the vesting period, which is considered to be the requisite service period. We record forfeitures in the periods in which they occur.
The fair value of share-based awards is estimated at the date of grant using the Black-Scholes option pricing model. The determination of the fair value of share-based awards is affected by our share price, as well as assumptions regarding a number of complex and subjective variables. Risk free interest rates are based upon United States Government bond rates appropriate for the expected term of each award. Expected volatility rates are based on the historical volatility over a term equal to the expected life of the option. The assumed dividend yield is zero, as we do not expect to declare any dividends in the foreseeable future. The expected term of options is estimated considering the vesting period at the grant date, the life of the option and the average length of time similar grants have remained outstanding in the past.
Warrants
We account for common share purchase warrants as either equity instruments or as liabilities depending on the specific terms of the warrant agreements. Generally, warrants are classified as equity, as opposed to liabilities, as the agreements do not include the potential for a cash settlement or an adjustment to the exercise price and are therefore deemed to be indexed to the Company’s own shares. Certain of the Company’s common share purchase warrants which matured in February 2018 were deemed to be derivative instruments and required to be reported at fair value. The fair value of common share purchase warrants is disclosed in Note 10 titled “Warrant Liability.”
Income taxes
Income taxes are accounted for under the asset and liability method. Deferred tax assets and liabilities are recognized for the estimated future tax consequences attributable to differences between the consolidated financial statement carrying amounts of existing assets and liabilities and their respective tax bases and operating loss and tax credit carry-forwards. Deferred tax assets and liabilities are measured using enacted rates, for each of the jurisdictions in which the Company operates, expected to apply to taxable income in the years in which those temporary differences are expected to be recovered or settled. The effect on deferred tax assets and liabilities of a change in tax rates is recognized in operations in the period that includes the enactment date. Valuation allowances are established when necessary to reduce deferred tax assets to the amount that is more likely than not to be realized. The Company has provided a full valuation allowance against the gross deferred tax assets as of December 31, 2019 and 2018. See Note 16, “Income Taxes” for additional information. The Company’s policy is to classify interest and penalties related to income taxes as income tax expense.
Government assistance
Government assistance relating to research and development performed by DiaMedica Australia Pty Ltd. is recorded as a component of Other (income) expense. Government assistance is recognized when the related expenditures are incurred. We recognized $856,000 and $621,000 of other income related to research activities performed in 2019 and 2018, respectively.
Net loss per share
We compute net loss per share by dividing our net loss (the numerator) by the weighted-average number of common shares outstanding (the denominator) during the period. Shares issued during the period and shares reacquired during the period, if any, are weighted for the portion of the period that they were outstanding. The computation of diluted earnings per share, or EPS, is similar to the computation of basic EPS except that the denominator is increased to include the number of additional common shares that would have been outstanding if the dilutive potential common shares had been issued. Our diluted EPS is the same as basic EPS due to the exclusion of common share equivalents as their effect would be anti-dilutive.
The following table summarizes our calculation of net loss per common share for the periods presented (in thousands, except share and per share data):
|
Year Ended December 31, |
||||||||
|
2019 |
2018 |
|||||||
|
Net loss |
$ | (10,649 | ) | $ | (5,734 | ) | ||
|
Weighted average shares outstanding—basic and diluted |
11,987,696 | 7,743,520 | ||||||
|
Basic and diluted net loss per share |
$ | (0.89 | ) | $ | (0.74 | ) | ||
The following outstanding potential common shares were not included in the diluted net loss per share calculations as their effects were not dilutive:
|
Year Ended December 31, |
||||||||
|
2019 |
2018 |
|||||||
|
Employee and non-employee stock options |
1,220,359 | 639,359 | ||||||
|
Common shares issuable under common share purchase warrants |
971,953 | 807,563 | ||||||
|
Common shares issuable under deferred unit plan |
21,183 | 21,183 | ||||||
| 2,213,495 | 1,468,105 | |||||||
Recently adopted accounting pronouncements
In May 2014, the Financial Accounting Standards Board (FASB) issued a new accounting standard that amended the guidance for the recognition of revenue from contracts with customers to transfer goods and services. The FASB subsequently issued additional, clarifying standards to address issues arising from implementation of the new revenue recognition standard. The new revenue recognition standard and clarifying standards require an entity to recognize revenue when control of promised goods or services is transferred to the customer at an amount that reflects the consideration to which the entity expects to be entitled in exchange for those goods or services. We adopted this new standard as of January 1, 2018. The adoption as of this date had no impact on our consolidated financial statements, as we had no revenue until the third quarter of 2018. We followed ASC 606, “Revenue from Contracts with Customers” in accounting for our former license and collaboration agreement with Ahon Pharmaceutical Co Ltd. (Note 13).
In February 2016, the FASB issued Accounting Standards Update (ASU) No. 2016-02, Leases. The guidance in ASU 2016-02 supersedes the lease recognition requirements in the Accounting Standards Codification Topic 840, Leases. ASU 2016-02 requires an entity to recognize assets and liabilities arising from a lease for both financing and operating leases, along with additional qualitative and quantitative disclosures. The new standard requires the immediate recognition of all excess tax benefits and deficiencies in the income statement and requires classification of excess tax benefits as an operating activity as opposed to a financing activity in the statements of cash flows. This standard became effective for us on January 1, 2019.
The FASB has subsequently issued the following amendments to ASU 2016-02, which have the same effective date and transition date of January 1, 2019, and which we collectively refer to as the new leasing standards:
|
● |
ASU No. 2018-01, Leases (Topic 842): Land Easement Practical Expedient for Transition to Topic 842, which permits an entity to elect an optional transition practical expedient to not evaluate under Topic 842 land easements that existed or expired prior to adoption of Topic 842 and that were not previously accounted for as leases under the prior standard, ASC 840, Leases. |
|
● |
ASU No. 2018-10, Codification Improvements to Topic 842, Leases, which amends certain narrow aspects of the guidance issued in ASU 2016-02. |
|
● |
ASU No. 2018-11, Leases (Topic 842): Targeted Improvements, which allows for a transition approach to initially apply ASU 2016-02 at the adoption date and recognize a cumulative-effect adjustment to the opening balance of retained earnings in the period of adoption as well as an additional practical expedient for lessors to not separate non-lease components from the associated lease component. |
|
● |
ASU No. 2018-20, Narrow-Scope Improvements for Lessors, which contains certain narrow scope improvements to the guidance issued in ASU 2016-02. |
We adopted the new leasing standards on January 1, 2019, using a modified retrospective transition approach to be applied to leases existing as of, or entered into after, January 1, 2019; and, consequently, financial information will not be updated and the disclosures required under Topic 842 will not be provided for dates and periods prior to January 1, 2019. We have reviewed our existing lease contracts and the impact of the new leasing standards on our consolidated results of operations, financial position and disclosures. Upon adoption of the new leasing standards, we recognized a lease liability and related right-of-use asset on our consolidated balance sheet of approximately $205,000.
In June 2018, the FASB issued ASU No. 2018-07, “Improvements to Nonemployee Share-Based Payment Accounting,” to simplify the accounting for share-based payments to nonemployees by aligning it with the accounting for share-based payments to employees, with certain exceptions. This ASU is effective for public entities for fiscal years beginning after December 15, 2018. Prior to the adoption of this ASU, share-based compensation awarded to non-employees was subject to revaluation over its vesting terms. Subsequent to the adoption of this ASU, non-employee share-based payment awards are measured on the date of grant, similar to share-based payment awards granted to employees. We adopted this standard on January 1, 2019 and the adoption of this ASU did not have a material impact on our financial position or our consolidated statements of operations.
|
4. |
Amounts Receivable |
Amounts receivable consisted of the following (in thousands):
|
December 31, 2019 |
December 31, 2018 |
|||||||
|
Research and development incentives |
$ | 793 | $ | 622 | ||||
|
Sales-based taxes receivable |
13 | 134 | ||||||
|
Other |
17 | 24 | ||||||
|
Total amounts receivable |
$ | 823 | $ | 780 | ||||
|
5. |
Marketable Securities |
The available-for-sale marketable securities are primarily comprised of investments in commercial paper, corporate bonds and government securities and consist of the following, measured at fair value on a recurring basis:
|
Fair Value Measurements as of December 31, 2019 Using Inputs Considered as |
||||||||||||||||
|
Fair Value |
Level 1 |
Level 2 |
Level 3 |
|||||||||||||
|
Commercial paper and corporate bonds |
$ | 1,997 | $ | — | $ | 1,997 | $ | — | ||||||||
|
Government securities |
1,998 | — | 1,998 | — | ||||||||||||
|
Total marketable securities |
$ | 3,995 | $ | — | $ | 3,995 | $ | — | ||||||||
Accrued interest receivable on available-for-sale securities was $25,000 as of December 31, 2019 and is included in amounts receivable.
There were no transfers of assets between Level 1 and Level 2 of the fair value measurement hierarchy during the year ended December 31, 2019.
Under the terms of the Company’s investment policy, purchases of marketable securities are limited to investment grade governmental and corporate obligations with a primary objective of principal preservation. Maturities of individual securities are less than one year and the amortized cost of all securities approximated fair value as of December 31, 2019.
|
6. |
Deposits |
Deposits consisted of the following (in thousands):
|
December 31, 2019 |
December 31, 2018 |
|||||||
|
Advances to vendors, current |
$ | 88 | $ | — | ||||
|
Advances to vendors, non-current |
$ | — | $ | 271 | ||||
We periodically advance funds to vendors engaged to support the performance of our clinical trials and related supporting activities. The funds advanced are held, interest free, for varying periods of time and may be recovered by DiaMedica through partial reductions of ongoing invoices, application against final study/project invoices or refunded upon completion of services to be provided. Deposits are classified as current or non-current based upon their expected recovery time.
|
7. |
Property and Equipment |
Property and equipment consisted of the following (in thousands):
|
December 31, 2019 |
December 31, 2018 |
|||||||
|
Furniture and equipment |
$ | 51 | $ | 49 | ||||
|
Computer equipment |
56 | 71 | ||||||
| 107 | 120 | |||||||
|
Less accumulated depreciation |
(43 | ) | (24 | ) | ||||
|
Property and equipment, net |
$ | 64 | $ | 96 | ||||
Depreciation expense for the years ended December 31, 2019 and 2018 was $21,000 and $15,000, respectively. During 2019 and 2018, we disposed of $14,000 and $17,000 of equipment, respectively.
|
8. |
Accounts Payable and Accrued Liabilities |
Accounts payable and accrued liabilities consisted of the following (in thousands):
|
December 31, 2019 |
December 31, 2018 |
|||||||
|
Trade and other payables |
$ | 182 | $ | 483 | ||||
|
Accrued clinical study costs |
433 | 292 | ||||||
|
Accrued compensation |
419 | 417 | ||||||
|
Accrued research and other professional fees |
172 | 65 | ||||||
|
Accrued taxes and other liabilities |
52 | 34 | ||||||
|
Total accrued liabilities |
$ | 1,258 | $ | 1,291 | ||||
|
9. |
Operating Lease |
We lease certain office space under a non-cancelable operating lease. This lease does not have significant rent escalation holidays, concessions, leasehold improvement incentives or other build-out clauses. Further this lease does not contain contingent rent provisions. This lease terminates on August 31, 2022 and we do not have an option to renew. This lease does include both lease (e.g., fixed rent) and non-lease components (e.g., common-area and other maintenance costs). The non-lease components are deemed to be executory costs and are therefore excluded from the minimum lease payments used to determine the present value of the operating lease obligation and related right-of-use asset.
This lease does not provide an implicit rate and, due to the lack of a commercially salable product, we are generally considered unable to obtain commercial credit. Therefore, considering the quoted rates for the lowest investment-grade debt and the interest rates implicit in recent financing leases, we estimated our incremental borrowing rate to be 9%. We used our estimated incremental borrowing rate and other information available at the lease commencement date in determining the present value of the lease payments.
Our operating lease cost and variable lease costs were $65,000 and $54,000, respectively, for the year ended December 31, 2019. Variable lease costs consist primarily of common area maintenance costs, insurance and taxes which are paid based upon actual costs incurred by the lessor.
Maturities of our operating lease obligation are as follows as of December 31, 2019 (in thousands):
|
2020 |
$ | 66 | ||
|
2021 |
68 | |||
|
2022 |
46 | |||
|
Total lease payments |
$ | 180 | ||
|
Less interest portion |
(21 | ) | ||
|
Present value of lease obligation |
$ | 159 |
|
10. |
Warrant Liability |
In February 2016, we completed, a non-brokered private placement of 234,375 units with each unit consisting of one common share and one half of one common share purchase warrant. Accordingly, we issued 117,188 warrants. In conjunction with this offering, the Company also issued an aggregate of 10,915 compensation warrants. Each warrant entitled the holder to purchase one common share at a price of CAD$5.00 at any time prior to expiry in February 2018.
As the warrant exercise price was stated in Canadian dollars and not the Company’s functional currency, the warrants were deemed to be derivative instruments. Accordingly, we recorded a warrant liability on the Company’s consolidated balance sheet for the initial estimated fair value of the warrants with subsequent changes in the estimated fair value recognized in the consolidated statements of operations and comprehensive loss. We allocated $281,000 of the net proceeds to the warrant liability and, for the compensation warrants, $24,000 was included in the issuance costs. The balance of the net proceeds were allocated to the common shares. The Company estimated the value of these warrants by using a Black-Scholes pricing model with the following assumptions: expected volatilities of 191.8 – 225.0%, risk-free interest rates of 0.43 – 0.49%, and expected life of 2 years.
During February 2018, 121,256 common shares were issued on the exercise of warrants for gross proceeds of approximately $483,000 and the remaining 4,346 warrants expired.
The fair values at the time of exercise of the warrants were estimated using the following valuation assumptions: expected volatilities of 16.7%, risk-free interest rates of 1.8%, and expected life of 0.01-0.03 years.
The following is a rollforward of the fair value of the warrants (in thousands):
|
Warrant Liability |
||||
|
Ending balance December 31, 2017 |
$ | 84 | ||
|
Change in fair value |
39 | |||
|
Exercises |
(123 | ) | ||
|
Ending balance December 31, 2018 |
$ | — | ||
|
11. |
Commitments and Contingencies |
Clinical trials and product development
In the normal course of business, the Company incurs obligations to make future payments as it executes its business plan. These contracts may relate to preclinical or clinical studies, manufacturing or manufacturing process development and other product development activities. Currently, these contracts include the clinical research organization conducting our Phase II clinical trial for acute ischemic stroke, clinical study sites in our Phase II CKD study and various vendors supporting the performance of these studies. These commitments are subject to significant change and the ultimate amounts due may be materially different as these obligations are affected by, among other factors, the number and pace of patients enrolled, the number of clinical study sites enrolling subjects, the amount of time to complete study enrollments and the time required to finalize, analyze and report of study results. Clinical research agreements are generally cancelable upon 30 days’ notice, with the Company’s obligation limited to costs incurred up to that date, including any non-cancelable costs. Cancelation terms for product manufacturing and process development contracts vary and are generally dependent upon timelines for sourcing research materials and reserving laboratory time. As of December 31, 2019, the Company estimates that its outstanding commitments, including such cancellable contracts, are approximately $4.9 million over the next 12 months and $0 in the following 12 months.
On September 11, 2017, we announced the initiation of REMEDY, a Phase II clinical trial evaluating DM199 in patients with acute ischemic stroke. The study drug (DM199 or placebo) was administered as an intravenous infusion within 24 hours of stroke symptom onset, followed by subcutaneous (under the skin) injections later that day and once every 3 days for 21 days. The study was designed to evaluate safety and tolerability of DM199 along with multiple tests designed to investigate DM199’s therapeutic potential including plasma-based biomarkers and standard functional stroke measures assessed at 90 days post-stroke (Modified Rankin Scale, National Institutes of Health Stroke Scale, Barthel Index, and C-reactive protein, a measure of inflammation). Enrollment completed in October 2019 and a total of 92 subjects were enrolled.
On December 17, 2019, we announced the enrollment of the first subject in REDUX, a multi-center, open-label, Phase II clinical trial investigating 60 participants with Stage II or III CKD, who will be enrolled in two equal cohorts. The study will evaluate two dose levels of DM199 within each cohort. Study participants will receive DM199 by subcutaneous injection twice weekly for 95 days. The primary study endpoints include safety, tolerability, blood pressure, albuminuria and kidney function, which will be evaluated by changes from baseline in the estimated glomerular flow rate (eGFR) and albuminuria, as measured by the urinary albumin to creatinine ratio (UACR).
Additional clinical trials will be subsequently required if the results of Phase II are positive. However, at this time, we are unable to reasonably estimate the total costs of future trials. Such costs are contingent on and subject to change depending on the results of current and future clinical trials as well as developments in the regulatory requirements.
Technology license
The Company has entered into a license agreement with Catalent Pharma Solutions, LLC (Catalent) whereby we have licensed certain gene expression technology and we contract with Catalent for the manufacture of DM199. Under the terms of this license, certain milestone and royalty payments may become due under this agreement and are dependent upon, among other factors, clinical trials, regulatory approvals and ultimately the successful development of a new drug, the outcome and timing of which is uncertain. As of December 31, 2019, two milestones remain which include $185,000 due upon the initiation of dosing in our first Phase III trial and $185,000 upon our first regulatory approval for commercial sale. Following the launch of our first product, we will also incur a royalty of less than 1% on net sales. The royalty term is indefinite but the license agreement may be canceled by us on 90 days’ prior written notice. The license may not be terminated by Catalent unless we fail to make required milestone and royalty payments. There were no amounts due or payable under this agreement during 2019 and 2018.
Litigation funding agreement
On December 27, 2019, we entered into a litigation funding agreement with LEGALIST FUND II, L.P. (Funder) for the purpose of funding our currently pending lawsuit against PRA Netherlands. Our management believes, but cannot guarantee, that this litigation funding agreement will allow us to pursue this litigation more effectively. Although the Funder made its evaluation as to the likelihood of success, litigation is very uncertain, and no assurance can be provided that, just because we have obtained litigation funding, we will be successful or that any recovery we may obtain will be significant.
Under the terms of the litigation funding agreement, the Funder agreed to pay up to an aggregate of $1.0 million to fund reasonable legal fees, court costs, and other expenses incurred by us in connection with the litigation, including $200,000 for fees and costs previously paid by us. These payments, however, are conditioned upon the transfer of venue of the litigation from Delaware to Minnesota (the Transfer) and if the venue is not transferred we will not be entitled to receive any payments under the litigation funding agreement. If the venue is transferred, we agreed to repay the Funder from any proceeds arising from the litigation (Claim Proceeds) the amount of costs actually paid or otherwise funded by the Funder in connection with the litigation, plus the reimbursement of $10,000 for its diligence and underwriting costs. Additionally, we agreed to pay the Funder from the Claim Proceeds the greater of: (i) $1.0 million if repayment occurs within nine months of the Transfer, $2.0 million if repayment occurs more than nine months after the Transfer but before trial has begun, or $3.0 million thereafter; or (ii) 20% of the Claim Proceeds. In the event the Funder has not been repaid 3½ years after the Transfer, the Funder is entitled to receive interest on the unpaid amounts equal to 20% per annum commencing on the 3½ year anniversary of the Transfer. Our obligation under the litigation funding agreement to make the foregoing payments to the Funder is non-recourse and limited only to the Claim Proceeds. As a result of the agreement, if we obtain Claim Proceeds, it is possible, depending on the amount of the Claim Proceeds, that we will receive no net recovery after all payments have been made to the Funder.
Indemnification of directors and officers
The Company, as permitted under laws of British Columbia and in accordance with the Company’s articles and indemnification agreements, will indemnify and advance expenses to its directors and officers to the fullest extent permitted by law and may choose to indemnify other employees or agents from time to time. The Company has secured insurance on behalf of any officer, director, employee or other agent for any liability arising out of his or her actions in connection with their services to the Company. As of December 31, 2019, there was no pending litigation or proceeding involving any director or officer of the Company as to which indemnification is required or permitted, and we are not aware of any threatened litigation or proceeding that may result in a claim for indemnification. Insofar as indemnification for liabilities arising under the United States Securities Act of 1933, as amended (Securities Act) may be permitted to directors, officers and controlling persons of the Company, the Company has been advised that, in the opinion of the United States Securities and Exchange Commission, such indemnification is against public policy as expressed in the Securities Act and is therefore unenforceable. The Company believes the fair value of these indemnification agreements is minimal. Accordingly, the Company had not recorded any liabilities for these obligations as of December 31, 2019 or 2018.
|
12. |
Shareholders’ Equity |
Authorized capital stock
DiaMedica has authorized share capital of an unlimited number of common voting shares and the shares do not have a stated par value.
Common shareholders are entitled to receive dividends as declared by the Company, if any, and are entitled to one vote per share at the Company's annual general meeting and any extraordinary general meeting.
Shareholders rights plan
The Company adopted a shareholder rights plan agreement (Rights Plan). The Rights Plan is designed to provide adequate time for the Board of Directors and the shareholders to assess an unsolicited takeover bid for the Company, to provide the Board of Directors with sufficient time to explore and develop alternatives for maximizing shareholder value if a takeover bid is made, and to provide shareholders with an equal opportunity to participate in a takeover bid and receive full and fair value for their common shares. The Rights Plan was renewed at the Company’s annual meeting of shareholders in December 2017 and is set to expire at the close of the Company’s annual meeting of shareholders in 2020.
The rights issued under the Rights Plan will initially attach to and trade with the common shares and no separate certificates will be issued unless an event triggering these rights occurs. The rights will become exercisable only when a person, including any related person or entity, acquires or attempts to acquire 20% or more of the outstanding common shares without complying with the “Permitted Bid” provisions of the Rights Plan or without approval of the Board of Directors. Should such an acquisition occur or be announced, each right would, upon exercise, entitle a rights holder, other than the acquiring person and related persons, to purchase common shares at a 50% discount to the market price at the time.
Under the Plan, a Permitted Bid is a bid made to all holders of the common shares and which is open for acceptance for not less than 60 days. If at the end of 60 days at least 50% of the outstanding common shares, other than those owned by the offeror and certain related parties have been tendered, the offeror may take up and pay for the common shares but must extend the bid for a further 10 days to allow other shareholders to tender.
The issuance of common shares upon the exercise of the rights is subject to receipt of certain regulatory approvals.
Equity issued during the year ended December 31, 2019
During the year ended December 31, 2019, 50,000 common shares were issued upon the exercise of options for gross proceeds of $75,000 and no warrants were exercised.
Equity issued during the year ended December 31, 2018
Public offering during 2018
On December 11, 2018, the Company issued and sold an aggregate of 4,100,000 common shares in an initial public offering at a price to the public of $4.00 per share. As a result of the offering, the Company received gross proceeds of $16.4 million, which resulted in net proceeds to the Company of approximately $14.7 million, after deducting the underwriting discount and offering expenses. None of the expenses associated with the initial public offering were paid to directors, officers, persons owning ten percent or more of any class of equity securities, or to their associates, or to our affiliates. On December 11, 2018, as additional underwriting compensation and in exchange for cash consideration of $50, the Company granted the underwriter a warrant to purchase 205,000 common shares (equal to 5.0% of the common shares sold in the initial public offering) at an exercise price of $4.80 per share (equal to 120% of the initial public offering price per common share in the initial public offering), subject to customary anti-dilution provisions. The warrant is exercisable for a term of five years. The warrant includes a cashless exercise provision entitling the underwriter to surrender a portion of the underlying common shares that has a value equal to the aggregate exercise price in lieu of paying cash upon exercise.
Private placements during 2018
On March 29, 2018, the Company completed, in two tranches, a brokered and non-brokered private placement of 1,322,965 units at a price of $4.90 per unit for aggregate gross proceeds of approximately $6.3 million. Each unit consisted of one common share and one half of one common share purchase warrant. The Company issued 661,482 warrants. Each warrant entitles the holder to purchase one common share at a price of $7.00 at any time prior to expiry on March 19, 2020 and March 29, 2020 for Tranche 1 and Tranche 2, respectively. The warrants are subject to early expiry under certain conditions. The warrant expiry date can be accelerated at the option of the Company, in the event that the volume-weighted average trading price of the Company’s common shares exceeds $12.00 per common share for any 21 consecutive trading days. In connection with this offering, the Company paid aggregate finder’s fees of approximately $384,000 and issued an aggregate of 80,510 compensation warrants. Each compensation warrant entitles the holder to purchase one common share at $4.90 for a period of 2 years from the closing of this offering, subject to acceleration on the same terms as the common share purchase warrants.
During the year ended December 31, 2018, 128,594 common shares were issued on the exercise of warrants for gross proceeds of $607,000 and 16,954 common shares were issued on the exercise of options for gross proceeds of $43,000.
Shares reserved
Common shares reserved for future issuance are as follows:
|
December 31, 2019 |
||||
|
Stock options outstanding |
1,220,359 | |||
|
Deferred share units outstanding |
21,183 | |||
|
Shares available for grant under the 2019 Omnibus Incentive Plan |
1,384,822 | |||
|
Common shares issuable under common share purchase warrants |
971,953 | |||
|
Total |
3,598,317 | |||
|
13. |
Former License and Collaboration Agreement with Related Party |
On September 27, 2018, the Company entered into a license and collaboration agreement (License Agreement) with Ahon Pharmaceutical Co Ltd. (Ahon Pharma), which granted Ahon Pharma exclusive rights to develop and commercialize DM199 for acute ischemic stroke in mainland China, Taiwan, Hong Kong S.A.R. and Macau S.A.R. Under the terms of the agreement, the Company received a non-refundable upfront payment of $500,000 upon signing the License Agreement and was entitled to receive an additional non-refundable payment of $4.5 million upon the earlier of regulatory clearance to initiate a clinical trial in China or July 1, 2019. The Company also had the potential to receive up to an additional $27.5 million in development and sales related milestones and up to approximately 10% royalties on net sales of DM199 in the licensed territories. All development, regulatory, sales, marketing and commercial activities and associated costs in the licensed territories were the sole responsibility of Ahon Pharma. By its terms, the License Agreement could be terminated at any time by Ahon Pharma by providing 120 days written notice.
On August 12, 2019, after extensive good faith discussions between Ahon Pharma and the Company, the parties were unable to agree upon mutually acceptable revised terms to the agreement and we terminated the License Agreement for non-payment of the $4.5 million milestone, thereby regaining worldwide rights to DM199 for acute ischemic stroke.
Ahon Pharma is a subsidiary of Shanghai Fosun Pharmaceutical (Group) co. Ltd. (Fosun Pharma) which, through its partnership with SK Group, a South Korea based company, is an investor in DiaMedica, holding approximately 8.3% of our common shares as of December 31, 2019. This investment was made in 2016.
|
14. |
Share-Based Compensation |
2019 Omnibus Incentive Plan
The DiaMedica Therapeutics Inc. 2019 Omnibus Incentive Plan (2019 Plan) was adopted by the Board of Directors in March 2019 and approved by our shareholders at our annual general and special meeting of shareholders held on May 22, 2019. The 2019 Plan permits the Board, or a committee or subcommittee thereof, to grant to the Company’s eligible employees, non-employee directors and consultants non-statutory and incentive stock options, stock appreciation rights, restricted stock awards, restricted stock units, deferred stock units, performance awards, non-employee director awards and other stock-based awards. We grant options to purchase common shares under the 2019 Plan at no less than the fair market value of the underlying common shares as of the date of grant. Options granted to employees and non-employee directors have a maximum term of ten years and generally vest in approximately equal quarterly installments over one to three years. Options granted to non-employees have a maximum term of five years and generally vest in approximately equal quarterly installments over one year. Subject to adjustment as provided in the 2019 Plan, the maximum number of the Company’s common shares authorized for issuance under the 2019 Plan is 2,000,000 shares. As of December 31, 2019, options to purchase 615,178 common shares were outstanding under the 2019 Plan.
Stock option plan
The DiaMedica Therapeutics Inc. Stock Option Plan, Amended and Restated November 6, 2018 (Prior Plan), was terminated by the Board of Directors in conjunction with the shareholder approval of the 2019 Plan. Awards outstanding under the Prior Plan remain outstanding in accordance with and pursuant to the terms thereof. Options granted under the Prior Plan have terms similar to those used under the 2019 Plan. As of December 31, 2019, options to purchase 605,181 common shares were outstanding under the Prior Plan.
Deferred share unit plan
The DiaMedica Therapeutics Inc. Amended and Restated Deferred Share Unit Plan (DSU Plan) was terminated by the Board of Directors in conjunction with the shareholder approval of the 2019 Plan. Awards outstanding under the DSU Plan remain outstanding in accordance with and pursuant to the terms thereof. As of December 31, 2019, there were 21,183 common shares reserved for deferred share units (DSUs) outstanding.
The aggregate number of common shares reserved for issuance for awards granted under the 2019 Plan, the Prior Plan and the DSU Plan as of December 31, 2019 was 1,241,542.
As the TSX Venture Exchange was the principal trading market for the Company’s common shares, all options granted prior to December 31, 2018 under the Prior Plan were priced in Canadian dollars. Options granted after December 31, 2018 under the 2019 Plan and the Prior Plan have been priced in United States dollars.
Share-based compensation expense for each of the periods presented is as follows (in thousands):
|
December 31, 2019 |
December 31, 2018 |
|||||||
|
Research and development |
$ | 370 | $ | 170 | ||||
|
General and administrative |
794 | 450 | ||||||
|
Total share-based compensation |
$ | 1,164 | $ | 620 | ||||
We recognize share-based compensation based on the fair value of each award as estimated using the Black-Scholes option valuation model. Ultimately, the actual expense recognized over the vesting period will only be for those shares that actually vest.
A summary of option activity is as follows (in thousands except share and per share amounts):
|
Shares Underlying Options |
Weighted Average Exercise Price Per Share |
Aggregate Intrinsic Value |
||||||||||
|
Balances at December 31, 2017 |
480,035 | $ | 4.98 | $ | 508 | |||||||
|
Granted |
196,800 | 8.55 | ||||||||||
|
Exercised |
(16,954 | ) | 2.54 | |||||||||
|
Expired/cancelled |
— | — | ||||||||||
|
Forfeited |
(20,522 | ) | 6.94 | |||||||||
|
Balances at December 31, 2018 |
639,359 | $ | 6.07 | $ | — | |||||||
|
Granted |
725,825 | 4.52 | ||||||||||
|
Exercised |
(50,000 | ) | 1.50 | |||||||||
|
Expired/cancelled |
(7,353 | ) | 5.49 | |||||||||
|
Forfeited |
(87,472 | ) | 5.22 | |||||||||
|
Balances at December 31, 2019 |
1,220,359 | $ | 5.33 | $ | 678 | |||||||
A summary of the status of our unvested shares during the year ended and as of December 31, 2019 is as follows:
|
Shares Underlying Options |
Weighted Grant Date Fair Value Per Share |
|||||||
|
Unvested at December 31, 2018 |
242,332 | $ | 5.75 | |||||
|
Granted |
725,825 | 3.21 | ||||||
|
Vested |
(301,938 | ) | 4.07 | |||||
|
Forfeited |
(87,472 | ) | 3.94 | |||||
|
Unvested at December 31, 2019 |
578,747 | $ | 3.73 | |||||
Information about stock options outstanding, vested and expected to vest as of December 31, 2019, is as follows:
|
Outstanding, Vested and Expected to Vest |
Options Vested and Exercisable |
|||||||||||||||||||||
|
Per Share Exercise Price |
Shares |
Weighted Average Remaining Contractual Life (Years) |
Weighted Average Exercise Price |
Options Exercisable |
Weighted Average Remaining Contractual Life (Years) |
|||||||||||||||||
| $2.00 |
- |
$2.99 | 132,900 | 6.0 | $ | 2.29 | 132,483 | 6.0 | ||||||||||||||
| $3.00 |
- |
$3.99 | 120,822 | 7.0 | 3.90 | 120,822 | 7.0 | |||||||||||||||
| $4.00 |
- |
$4.99 | 746,407 | 9.2 | 4.55 | 248,403 | 8.8 | |||||||||||||||
| $5.00 |
- |
$10.00 | 170,080 | 8.4 | 8.33 | 89,755 | 8.4 | |||||||||||||||
| $10.01 |
- |
$34.00 | 50,150 | 2.9 | 18.22 | 50,150 | 2.9 | |||||||||||||||
| 1,220,359 | 8.2 | $ | 5.33 | 641,613 | 7.3 | |||||||||||||||||
The cumulative grant date fair value of employee options vested during the years ended December 31, 2019 and 2018 was $918,000 and $508,000, respectively. Total proceeds received for options exercised during the years ended December 31, 2019 and 2018 were $75,000 and $43,000, respectively.
As of December 31, 2019, total compensation expense related to unvested employee stock options not yet recognized was $2.1 million, which is expected to be allocated to expenses over a weighted-average period of 2.3.
The aggregate intrinsic value of stock options exercised during the years ended December 31, 2019 and 2018 was $75,000 and $104,000, respectively.
The assumptions used in calculating the fair value under the Black-Scholes option valuation model are set forth in the following table for options issued by the Company for the years ended December 31, 2018 and 2017:
|
2019 |
2018 |
|||||||
|
Common share fair value |
$2.07 |
- | $4.60 | $6.82 |
- |
$7.20 | ||
|
Risk-free interest rate |
1.5 | – | 2.4% | 2.1 | – | 2.2% | ||
|
Expected dividend yield |
0% | 0% | ||||||
|
Expected option life |
4.2 | – | 5.1 | 4.8 | – | 5.0 | ||
|
Expected stock price volatility |
88.7 | – | 103.5% | 123.5 | – | 135.7% | ||
|
15. |
Employee Benefit Plan |
We maintain an employee 401(k) retirement savings plan (401(k) Plan). The 401(k) Plan provides eligible employees with an opportunity to make tax-deferred contributions into a long-term investment and savings program. All employees over the age of 21 may elect to participate in the 401(k) Plan beginning on their hire date. The 401(k) Plan allows eligible employees to contribute a portion of their annual compensation, subject only to maximum limits required by law. We contribute an amount up to 4% of each employees’ compensation under the safe harbor provisions provided by the Internal Revenue Service rules governing 401(k) plans. Employee and employer safe harbor contributions vest immediately.
We have recorded contribution expenses of $62,000 and $45,000 for the years ended December 31, 2019 and 2018, respectively.
|
16. |
Income Taxes |
The Company has incurred net operating losses since inception. The Company has not reflected the benefit of net operating loss carryforwards in the accompanying consolidated financial statements and has established a full valuation allowance against its deferred tax assets.
Deferred income taxes reflect the net tax effects of temporary differences between the carrying amounts of assets and liabilities for financial reporting purposes and the amounts used for income tax purposes as well as operating losses and tax credit carryforwards.
The significant components of our deferred tax assets and liabilities are as follows (in thousands):
|
December 31, |
||||||||
|
2019 |
2018 |
|||||||
|
Deferred tax assets (liabilities): |
||||||||
|
Non-capital losses carried forward |
$ | 11,211 | $ | 9,280 | ||||
|
Research and development expenditures |
817 | 887 | ||||||
|
Share issue costs |
395 | 529 | ||||||
|
Patents and other |
294 | 293 | ||||||
|
Accruals |
13 | (97 | ) | |||||
|
Property and equipment |
3 | (6 | ) | |||||
|
Total deferred tax asset, net |
12,733 | 10,886 | ||||||
|
Valuation allowance |
(12,733 | ) | (10,886 | ) | ||||
|
Net deferred tax asset |
$ | — | $ | — | ||||
Realization of the future tax benefits is dependent on our ability to generate sufficient taxable income within the carryforward period. Because of our history of operating losses, management believes that the deferred tax assets arising from the above-mentioned future tax benefits are currently not likely to be realized and, accordingly, we have provided a full valuation allowance.
The reconciliation of the Canadian statutory income tax rate applied to the net loss for the year to the income tax expense is as follows:
|
December 31, |
||||||||
|
2019 |
2018 |
|||||||
|
Statutory income tax rate |
27.0 | % | 27.0 | % | ||||
|
Income tax recovery based on statutory rate |
$ | (2,841 | ) | $ | (1,119 | ) | ||
|
Share-based compensation |
315 | 243 | ||||||
|
Gain on revaluation of warrant liability |
— | (450 | ) | |||||
|
Australian research and development incentive |
137 | 103 | ||||||
|
Other |
(9 | ) | 172 | |||||
|
Change in valuation allowance |
2,429 | 1,131 | ||||||
|
Income tax expense |
$ | 31 | $ | 80 | ||||
Net operating losses and tax credit carryforwards as of December 31, 2019, are as follows:
|
Amount (In thousands) |
Expiration Years |
||||
|
Non-capital income tax losses, net |
$ | 38,425 |
Beginning 2026 |
||
|
Research and development expense carry forwards |
3,026 |
Indefinitely |
|||
|
Tax credits |
484 |
Beginning 2020 |
|||
The Company is subject to taxation in the Canada, the United States and Australia. Tax returns, since the inception of DiaMedica Therapeutics Inc., are subject to examinations by Canadian tax authorities and may change upon examination. Tax returns of DiaMedica USA, Inc., since its inception in 2012 and thereafter, are subject to examination by the U.S. federal and state tax authorities. Tax returns of DiaMedica Therapeutics Australia Pty Ltd., since its inception in 2016 and thereafter, are subject to examination by the Australian tax authorities.
|
17. |
Subsequent Event |
On February 13, 2020, we issued and sold an aggregate of 2,125,000 common shares in a public, underwritten offering at a public offering price of $4.00 per share. As a result of the offering, we received gross proceeds of $8.5 million, which resulted in net proceeds to us of approximately $7.7 million, after deducting the underwriting discount and offering expenses. None of the expenses associated with the public offering were paid to directors, officers, persons owning ten percent or more of any class of equity securities, or to their associates, or to our affiliates.
|
Item 9. |
Changes In and Disagreements With Accountants on Accounting and Financial Disclosure |
None.
|
Item 9A. |
Controls and Procedures |
Evaluation of Disclosure Controls and Procedures
We maintain disclosure controls and procedures (as defined in Rules 13a-15(e) and 15d-15(e) under the United States Securities Exchange Act of 1934, as amended (Exchange Act)) that are designed to provide reasonable assurance that information required to be disclosed by us in the reports we file or submit under the Exchange Act, is recorded, processed, summarized and reported, within the time periods specified in the SEC’s rules and forms and that such information is accumulated and communicated to our management, including our principal executive officer and principal financial officer, or persons performing similar functions, as appropriate to allow timely decisions regarding required disclosure. Our management evaluated, with the participation of its Chief Executive Officer and its Chief Financial Officer, the effectiveness of the design and operation of our disclosure controls and procedures as of the end of the period covered in this report. Based on that evaluation, our Chief Executive Officer and Chief Financial Officer concluded that our disclosure controls and procedures were effective as of the end of such period to provide reasonable assurance that information required to be disclosed in the reports that we file or submit under the Exchange Act is recorded, processed, summarized and reported within the time periods specified in the SEC’s rules and forms, and that such information is accumulated and communicated to our management, including our Chief Executive Officer and Chief Financial Officer, as appropriate, to allow timely decisions regarding required disclosure.
Management’s Report on Internal Control over Financial Reporting
Management is responsible for establishing and maintaining adequate internal control over financial reporting, as such term is defined in Rule 13a-15(f) under the Exchange Act.
Our management conducted an assessment of the effectiveness of our internal control over financial reporting based on the criteria set forth in “Internal Control-Integrated Framework (2013)” issued by the Committee of Sponsoring Organizations of the Treadway Commission. Based on this assessment, management concluded that, as of December 31, 2019, our internal control over financial reporting was effective.
This Annual Report on Form 10-K does not include an attestation report of our independent registered public accounting firm on internal control over financial reporting due to an exemption established by the JOBS Act for “emerging growth companies.”
Changes in Internal Control over Financial Reporting
There was no change in our internal control over financial reporting that occurred during the fourth quarter ended December 31, 2019 that has materially affected or is reasonably likely to materially affect our internal control over financial reporting.
|
Item 9B. |
Other Information |
On February 21, 2020, the Compensation Committee approved the following officer payouts under the DiaMedica Therapeutics Inc. Short-Term Incentive Plan for 2019 performance, in each case representing 80% of the officer’s respective target bonus opportunity:
|
Officer Name and Position |
2019 Base Salary |
Target Incentive Percentage of Base Salary |
Target Bonus Opportunity |
2019 Actual Payout |
||||||||||||
|
Rick Pauls President and Chief Executive Officer |
$ | 445,000 | 50 | % | $ | 225,500 | $ | 178,000 | ||||||||
|
Scott Kellen Chief Financial Officer and Secretary |
270,000 | 30 | % | 81,000 | 64,800 | |||||||||||
|
Harry Alcorn, Jr., Pharm.D. Chief Medical Officer |
285,000 | 30 | % | 85,500 | 68,400 | |||||||||||
PART III
|
Item 10. |
Directors, Executive Officers and Corporate Governance |
Directors
The information in the “Voting Proposal One – Election of Directors” section of our definitive proxy statement to be filed with the SEC with respect to our next annual general meeting of shareholders, which involves the election of directors, is incorporated in this annual report on Form 10-K by reference.
Executive Officers
Information concerning our executive officers is included in this annual report on Form 10-K under Item 1 of Part I under “Information About Our Executive Officers.”
Code of Ethics
We have adopted a code of business conduct and ethics applicable to all of our directors, officers and employees, in accordance with Section 406 of the Sarbanes-Oxley Act, the rules of the SEC promulgated thereunder, and the Nasdaq Listing Rules. In the event that any changes are made or any waivers from the provisions of the code of business conduct and ethics are made, these events would be disclosed on our website or in a report on Form 8-K within four business days of such event. The code of business conduct and ethics is posted on our website at www.diamedica.com. Copies of the code of business conduct and ethics will be provided free of charge upon written request directed to Investor Relations, DiaMedica Therapeutics Inc., Two Carlson Parkway, Suite 260, Minneapolis, Minnesota 55447.
Changes to Nomination Procedures
During the fourth quarter of fiscal 2019, we made no material changes to the procedures by which shareholders may recommend nominees to the Company’s Board of Directors.
Audit Committee Matters
The information in the “Corporate Governance—Audit Committee” section of our definitive proxy statement to be filed with the SEC with respect to our next annual general meeting of shareholders, which involves the election of directors, is incorporated in this annual report on Form 10-K by reference.
|
Item 11. |
Executive Compensation |
The information in the “Director Compensation” and “Executive Compensation” sections of our definitive proxy statement to be filed with the SEC with respect to our next annual general meeting of shareholders, which involves the election of directors, is incorporated in this annual report on Form 10-K by reference.
|
Item 12. |
Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters |
Stock Ownership
The information in the “Stock Ownership—Security Ownership of Significant Beneficial Owners” and “Stock Ownership—Security Ownership of Management” sections of our definitive proxy statement to be filed with the SEC with respect to our next annual general meeting of shareholders, which involves the election of directors, is incorporated in this annual report on Form 10-K by reference.
Securities Authorized for Issuance under Equity Compensation Plans
The following table summarizes outstanding options and other awards under our equity compensation plans as of December 31, 2019. Our equity compensation plans as of December 31, 2019 were the DiaMedica Therapeutics Inc. 2019 Omnibus Incentive Plan (2019 Plan), the DiaMedica Therapeutics Inc. Stock Option Plan Amended and Restated November 6, 2018 (Prior Plan) and the DiaMedica Therapeutics Inc. Amended and Restated Deferred Share Unit Plan (DSU Plan).
|
(a) |
(b) |
(c) |
||||||||||
|
Plan Category |
Number of Securities to be Issued Upon Exercise of Outstanding Options, Warrants and Rights |
Weighted-Average Exercise Price of Outstanding Options, Warrants and Rights |
Number of Securities Remaining Available for Future Issuance Under Equity Compensation Plans (excluding securities reflected in column (a)) |
|||||||||
|
Equity compensation plans approved by security holders |
1,241,542 | (1) | $ | 5.32 | (2) | 1,384,822 | (3) | |||||
|
Equity compensation plans not approved by security holders |
— | $ | — | — | ||||||||
|
Total |
1,241,542 | (1) | $ | 5.32 | (2) | 1,384,822 | (3) | |||||
|
(1) |
Amount includes 615,178 common shares issuable upon the exercise of stock options outstanding under the 2019 Plan, 605,181 common shares issuable upon the exercise of stock options under the Prior Plan and 21,183 common shares issuable under the DSU Plan. |
|
(2) |
Not included in the weighted-average exercise price calculation are the 21,183 deferred share unit awards under the DSU Plan. |
|
(3) |
Amount includes 1,384,822 shares remaining available for future issuance under the 2019 Plan. |
|
Item 13. |
Certain Relationships and Related Transactions, and Director Independence |
The information in the “Related Person Relationships and Transactions” and “Corporate Governance—Director Independence” sections of our definitive proxy statement to be filed with the SEC with respect to our next annual general meeting of shareholders, which involves the election of directors, is incorporated in this annual report on Form 10-K by reference.
|
Item 14. |
Principal Accounting Fees and Services |
The information in the “Voting Proposal Two—Appointment of Baker Tilly Virchow Krause, LLP as our Independent Registered Public Accounting Firm and Authorization to Fix Remuneration” section of our definitive proxy statement to be filed with the SEC with respect to our next annual general meeting of shareholders, which involves the election of directors, is incorporated in this annual report on Form 10-K by reference.
PART IV
|
Item 15. |
Exhibits, Financial Statement Schedules |
Financial Statements
Our consolidated financial statements are included in “Part II, Item 8. Financial Statements and Supplementary Data.”
Financial Statement Schedules
All financial statement schedules are omitted because they are inapplicable since we are a smaller reporting company.
Exhibits
The exhibits being filed or furnished with this report are listed below, along with an indication as to each management contract or compensatory plan or arrangement.
A copy of any of the exhibits listed or referred to herein will be furnished at a reasonable cost to any person who is a shareholder upon receipt from any such person of a written request for any such exhibit. Such request should be sent to: Mr. Scott Kellen, Chief Financial Officer and Corporate Secretary, DiaMedica Therapeutics Inc., Two Carlson Parkway, Suite 260, Minneapolis, Minnesota 55447, Attn: Shareholder Information.
|
Item No. |
Item |
Method of Filing |
|
3.1 |
Notice of Articles of DiaMedica Therapeutics Inc. dated May 31, 2019 |
Incorporated by reference to Exhibit 3.1 to DiaMedica’s Current Report on Form 8-K as filed with the Securities and Exchange Commission on June 4, 2019 (File No. 001-36291)
|
|
3.2 |
Incorporated by reference to Exhibit 3.2 to DiaMedica’s Current Report on Form 8-K as filed with the Securities and Exchange Commission on June 4, 2019 (File No. 001-36291)
|
|
|
4.1 |
Description of Securities Registered Pursuant to Section 12 of the Securities Exchange Act of 1934 |
Filed herewith
|
|
4.2 |
Specimen Certificate representing Voting Common Shares of DiaMedica Therapeutics Inc. |
Incorporated by reference to Exhibit 4.2 to DiaMedica’s Current Report on Form 8-K as filed with the Securities and Exchange Commission on June 4, 2019 (File No. 001-36291)
|
| Item No. | Item | Method of Filing |
|
4.3 |
Incorporated by reference to Exhibit 4.2 to DiaMedica’s Registration Statement on Form S-1 as filed with the Securities and Exchange Commission on November 9, 2018 (File No. 333-228313)
|
|
|
4.4 |
Investment Agreement dated July 16, 2016 between Hermeda Industrial Co., Ltd. and DiaMedica Inc. |
Incorporated by reference to Exhibit 4.1 to DiaMedica’s Registration Statement on Form S-1 as filed with the Securities and Exchange Commission on November 9, 2018 (File No. 333-228313)
|
|
4.5 |
Form of Investor Warrant issued in connection with the March 2018 private placement |
Incorporated by reference to Exhibit 4.9 to DiaMedica’s Registration Statement on Form S-1 as filed with the Securities and Exchange Commission on November 9, 2018 (File No. 333-228313)
|
|
4.6 |
Form of Broker Warrant issued in connection with the March 2018 private placement |
Incorporated by reference to Exhibit 4.10 to DiaMedica’s Registration Statement on Form S-1 as filed with the Securities and Exchange Commission on November 9, 2018 (File No. 333-228313)
|
|
4.7 |
Incorporated by reference to Exhibit 10.1 to DiaMedica’s Current Report on Form 8-K as filed with the Securities and Exchange Commission on December 11, 2018
|
|
|
4.8 |
|
Filed herewith |
|
10.1# |
Incorporated by reference to Exhibit 10.1 to DiaMedica’s Current Report on Form 8-K as filed with the Securities and Exchange Commission on May 23, 2019 (File No. 001-36291)
|
| Item No. | Item | Method of Filing |
|
10.2# |
Form of Option Award Agreement under the DiaMedica Therapeutics Inc. 2019 Omnibus Incentive Plan |
Incorporated by reference to Exhibit 10.2 to DiaMedica’s Current Report on Form 8-K as filed with the Securities and Exchange Commission on June 21, 2019 (File No. 001-36291)
|
|
10.3# |
Incorporated by reference to Exhibit 10.3 to DiaMedica’s Current Report on Form 8-K as filed with the Securities and Exchange Commission on June 21, 2019 (File No. 001-36291)
|
|
|
10.4# |
DiaMedica Therapeutics Inc. Stock Option Plan Amended and Restated November 6, 2018 |
Incorporated by reference to Exhibit 10.1 to DiaMedica’s Registration Statement on Form S-1 as filed with the Securities and Exchange Commission on November 9, 2018 (File No. 333-228313)
|
|
10.5# |
Incorporated by reference to Exhibit 10.3 to DiaMedica’s Registration Statement on Form S-1 as filed with the Securities and Exchange Commission on November 9, 2018 (File No. 333-228313)
|
|
|
10.6# |
Incorporated by reference to Exhibit 10.2 to DiaMedica’s Registration Statement on Form S-1 as filed with the Securities and Exchange Commission on November 9, 2018 (File No. 333-228313)
|
|
|
10.7# |
DiaMedica Therapeutics Inc. Amended and Restated Deferred Share Unit Plan |
Incorporated by reference to Exhibit 10.4 to DiaMedica’s Registration Statement on Form S-1 as filed with the Securities and Exchange Commission on November 9, 2018 (File No. 333-228313)
|
|
10.8# |
Incorporated by reference to Exhibit 10.1 to DiaMedica’s Current Report on Form 8-K as filed with the Securities and Exchange Commission on June 21, 2019 (File No. 001-36291)
|
| Item No. | Item | Method of Filing |
|
10.9# |
Form of Indemnification Agreement between DiaMedica Therapeutics Inc. and Each Director and Officer |
Incorporated by reference to Exhibit 10.1 to DiaMedica’s Current Report on Form 8-K as filed with the Securities and Exchange Commission on June 4, 2019 (File No. 001-36291)
|
|
10.10# |
Incorporated by reference to Exhibit 10.6 to DiaMedica’s Registration Statement on Form S-1 as filed with the Securities and Exchange Commission on November 9, 2018 (File No. 333-228313)
|
|
|
10.11# |
Incorporated by reference to Exhibit 10.7 to DiaMedica’s Annual Report on Form 10-K for the year ended December 31, 2018 (File No. 001-36291)
|
|
|
10.12# |
Incorporated by reference to Exhibit 10.9 to DiaMedica’s Annual Report on Form 10-K for the year ended December 31, 2018 (File No. 001-36291)
|
|
|
10.13 |
Incorporated by reference to Exhibit 10.8 to DiaMedica’s Registration Statement on Form S-1 as filed with the Securities and Exchange Commission on November 9, 2018 (File No. 333-228313)
|
|
|
10.14 |
Incorporated by reference to Exhibit 10.9 to DiaMedica’s Registration Statement on Form S-1 as filed with the Securities and Exchange Commission on November 9, 2018 (File No. 333-228313)
|
|
|
10.15 |
First Amendment to Lease dated May 3, 2017 between One Two Holdings LLC and DiaMedica USA Inc. |
Incorporated by reference to Exhibit 10.10 to DiaMedica’s Registration Statement on Form S-1 as filed with the Securities and Exchange Commission on November 9, 2018 (File No. 333-228313)
|
| Item No. | Item | Method of Filing |
|
10.16 |
Incorporated by reference to Exhibit 10.11 to DiaMedica’s Registration Statement on Form S-1 as filed with the Securities and Exchange Commission on November 9, 2018 (File No. 333-228313)
|
|
|
10.17(1) |
Incorporated by reference to Exhibit 10.12 to DiaMedica’s Registration Statement on Form S-1 as filed with the Securities and Exchange Commission on November 9, 2018 (File No. 333-228313)
|
|
|
10.18 |
Incorporated by reference to Exhibit 10.13 to DiaMedica’s Registration Statement on Form S-1 as filed with the Securities and Exchange Commission on November 9, 2018 (File No. 333-228313)
|
|
|
10.19 |
Filed herewith
|
|
|
10.20 |
Incorporated by reference to Exhibit 10.1 to DiaMedica’s Current Report on Form 8-K as filed with the Securities and Exchange Commission on January 3, 2020 (File No. 001-36291)
|
|
|
21.1 |
Filed herewith
|
|
|
23.1 |
Filed herewith
|
|
|
31.1 |
|
Filed herewith
|
|
31.2 |
Filed herewith
|
|
|
32.1 |
Furnished herewith
|
| Item No. | Item | Method of Filing |
|
32.2 |
Furnished herewith
|
|
|
101 |
The following materials from DiaMedica Therapeutics Inc.’s Annual Report on Form 10-K for the year ended December 31, 2019, formatted in XBRL (Extensible Business Reporting Language): (i) the Consolidated Balance Sheets, (ii) the Consolidated Statements of Operations, (iii) the Consolidated Statements of Comprehensive Income (Loss), (iv) the Consolidated Statements of Equity, (v) the Consolidated Statements of Cash Flows, and (vi) Notes to Consolidated Financial Statements |
Filed herewith
|
| # | Indicates a management contract or compensatory plan or arrangement. |
|
(1) |
Portions of this exhibit have been redacted and are subject to an order granting confidential treatment under Rule 406 of the United States Securities Act of 1933, as amended (File No. 333-228313, CF #36833). The redacted material was filed separately with the Securities and Exchange Commission. |
|
Item 16. |
Form 10-K Summary |
None.
SIGNATURES
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned, thereunto duly authorized.
|
|
DIAMEDICA THERAPEUTICS INC. |
|
|
|
|
|
|
|
|
|
|
|
|
|
Date: March 23, 2020 |
By: |
/s/ Rick Pauls |
|
|
|
|
Rick Pauls |
|
|
|
|
President and Chief Executive Officer |
|
Pursuant to the requirements of the Securities Exchange Act of 1934, this report has been signed below by the following persons on behalf of the registrant and in the capacities and on the dates indicated.
|
Name |
Title |
Date |
||
|
/s/ Rick Pauls |
President, Chief Executive Officer and Director |
March 23, 2020 |
||
| Rick Pauls | (principal executive officer) | |||
|
/s/ Scott Kellen |
Chief Financial Officer and Secretary |
March 23, 2020 |
||
| Scott Kellen | (principal financial and accounting officer) | |||
|
/s/ Richard Pilnik |
Chairman of the Board |
March 23, 2020 |
||
| Richard Pilnik | ||||
|
/s/ Michael Giuffre, M.D. |
Director |
March 23, 2020 |
||
| Michael Giuffre, M.D. | ||||
|
/s/ James Parsons |
Director |
March 23, 2020 |
||
| James Parsons | ||||
|
/s/ Zhenyu Xiao, Ph.D. |
Director |
March 23, 2020 |
||
| Zhenyu Xiao, Ph.D. |
[page intentionally left blank]